This is tabbed text.
Here’s another indented line.
Cyto ─ Contents
Classification, Papanicolaou Society 2014
Benign / Negative (for Malignancy)
Chronic Pancreatitis & Reactive Ductal Atypia
Groove/paraduodenal pancreatitis
Autoimmune and IgG4-related pancreatitis
Pancreaticobiliary neoplasm (low & high risk)
Pancreatic intraepithelial neoplasia
Biliary intraepithelial neoplasia
Pancreatic intraductal papillary mucinous neoplasm
Intraductal papillary neoplasm of the bile duct
Intraductal oncocytic papillary neoplasm
Intraductal tubulopapillary neoplasm
Other WHO low-risk lesions (including spindle cell tumours)
Solid Pseudopapillary Neoplasm
Pancreatic Ductal Adenocarcinoma
Contaminants and miscellaneous
Atypia of undetermined significance
Follicular neoplasm ─ oncocytic
Encapsulated Follicular Variant PTC and NIFTP
Follicular Variant PTC with Infiltrative Growth
Cribriform morular thyroid carcinoma
Atypia of unknown significance
Metastatic Urothelial Carcinoma
Bronchial brushing and bronchial washing
I ─ Insufficient / Inadequate / Non-diagnostic
Pulmonary alveolar proteinosis
Solitary tracheobronchial papilloma
Basal cell hyperplasia / Reserve cell hyperplasia
Reactive bronchial epithelium, repair and regeneration
Cytopathic changes in viral infection
Chemotherapy- and radiotherapy-related changes
IV ─ Suspicious for Malignancy
Squamous cell carcinoma ─ well diff
Squamous cell carcinoma ─ mod to poorly diff
Large cell neuroendocrine carcinoma
Pulmonary Langerhans cell histiocytosis
Non-Neoplastic, Non-Infectious Diseases
Granulomatosis with Polyangiitis
Pulmonary Alveolar Proteinosis
Lactating adenoma/lactational change
─ Cyto ─ Pancreas
Media cytology pathoutlines
Classification, Papanicolaou Society 2014
I non-diagnostic
II negative
III atypical
IV neoplastic benign or other (WD-NET)
V suspicious
VI malignant PDAC, acinar cell CA, NEC
Classification, WHO
Media WHO pathoutlines
Non-Diagnostic
micro histiocytes only
no background mucin (mucinous cyst)
no hematoidin & mixed inflm (pseudocyst)
note biochemical tests not perormed (CEA, glucose)
molecular analysis may be informative
❌ "Non-diagnostic", reasons include:
Presence of atypia precludes this category
Preparation artefact ─ degeneration & stain precipitate
Obscuring blood
Contaminant GI epithelium
Normal pancreatic tissue in the context of a mass
Acellular in the context of a solid mass
Acellular and non-mucinous in the context of a cyst
Benign / Negative (for Malignancy)
def unequivocally benign cytopathology
note may or may not be specifically diagnostic
benign lymphangioma, serous cystadenoma
non-neoplastic chronic pancreatitis, pseudocyst, others
Atypical
def predominantly benign cytopathology
minimally malignant cytopathology
note PaN_Low, PaN_High, or malignant process
atypical cyst fluid non-thick mucin
atypical cells that cannot be distinguished from contaminants GIT with degeneration inconclusive biochemical analysis
Normal and contaminants
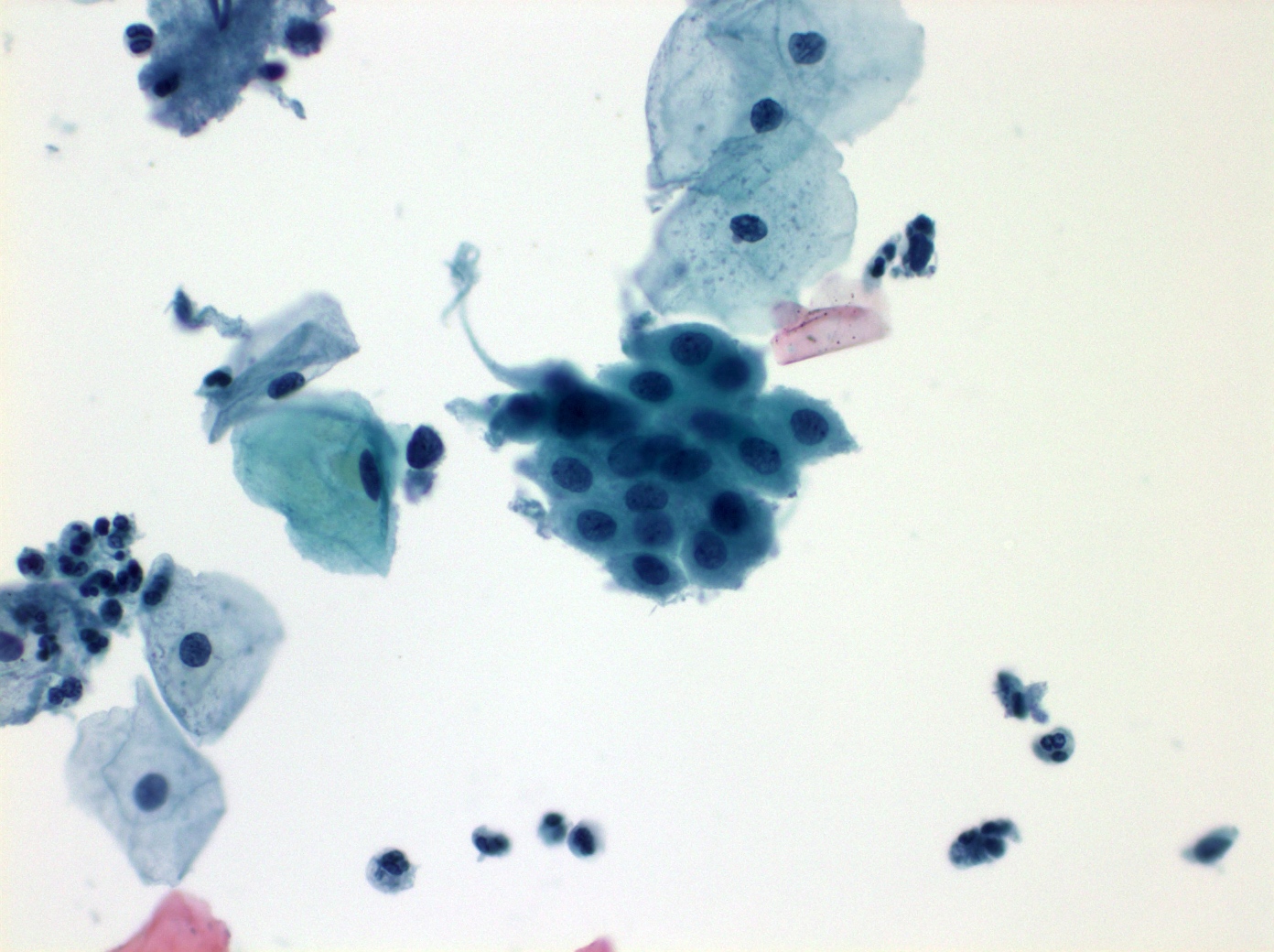
Benign Acinar Cells
cytology cohesive aggregates attached to FVS
~grapes on a vine
nucleus round to oval, most eccentric, some naked[1]
nucleolus prominent, bigger if reactive
chromatin evenly distributed, finely granular
cell borders indistinct
cytoplasm abundant & granular
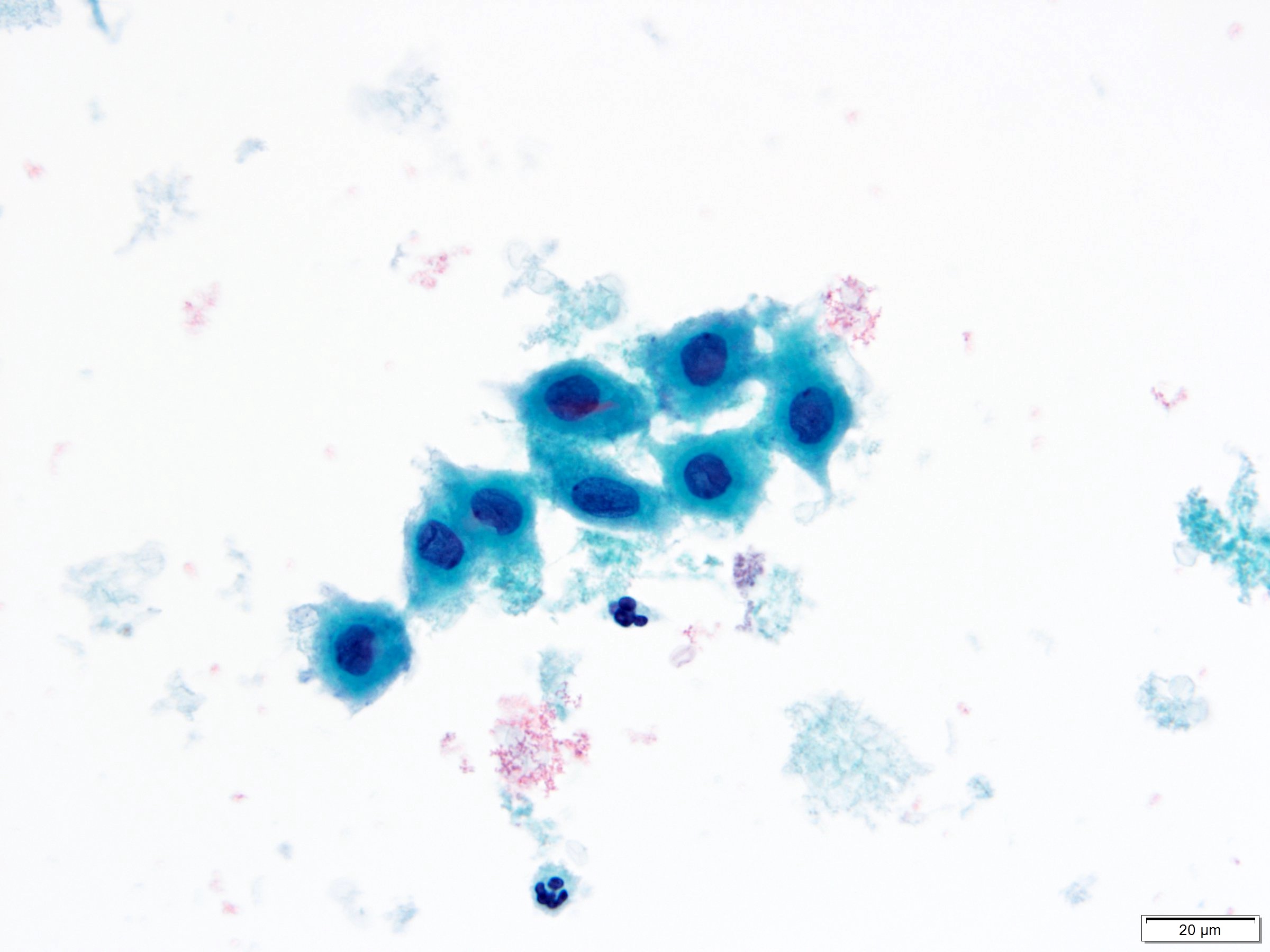
Benign Ductal Cells
cytology cohesive flat sheets
~honeycomb
nucleus round to oval, evenly distributed
nucleolus inconspicuous
chromatin evenly distributed, finely granular
cell borders distinct
note unlike larger mesothelial cells, lack windows
Background Duodenal Mucosa
cytology honeycomb monolayer papillary groups (villi)
nonmucinous glandular cells with brush border
sporadic goblet cells ~fried eggs
scattered lymphocytes in epithelium ~sesame seeds
note common contaminant in EUS-FNA
Background Gastric Mucosa
cytology small sheets & strips gastric crypts
mucin-capped foveolar cells, no brush border
grooved naked nuclei
note common contaminant in EUS-FNA
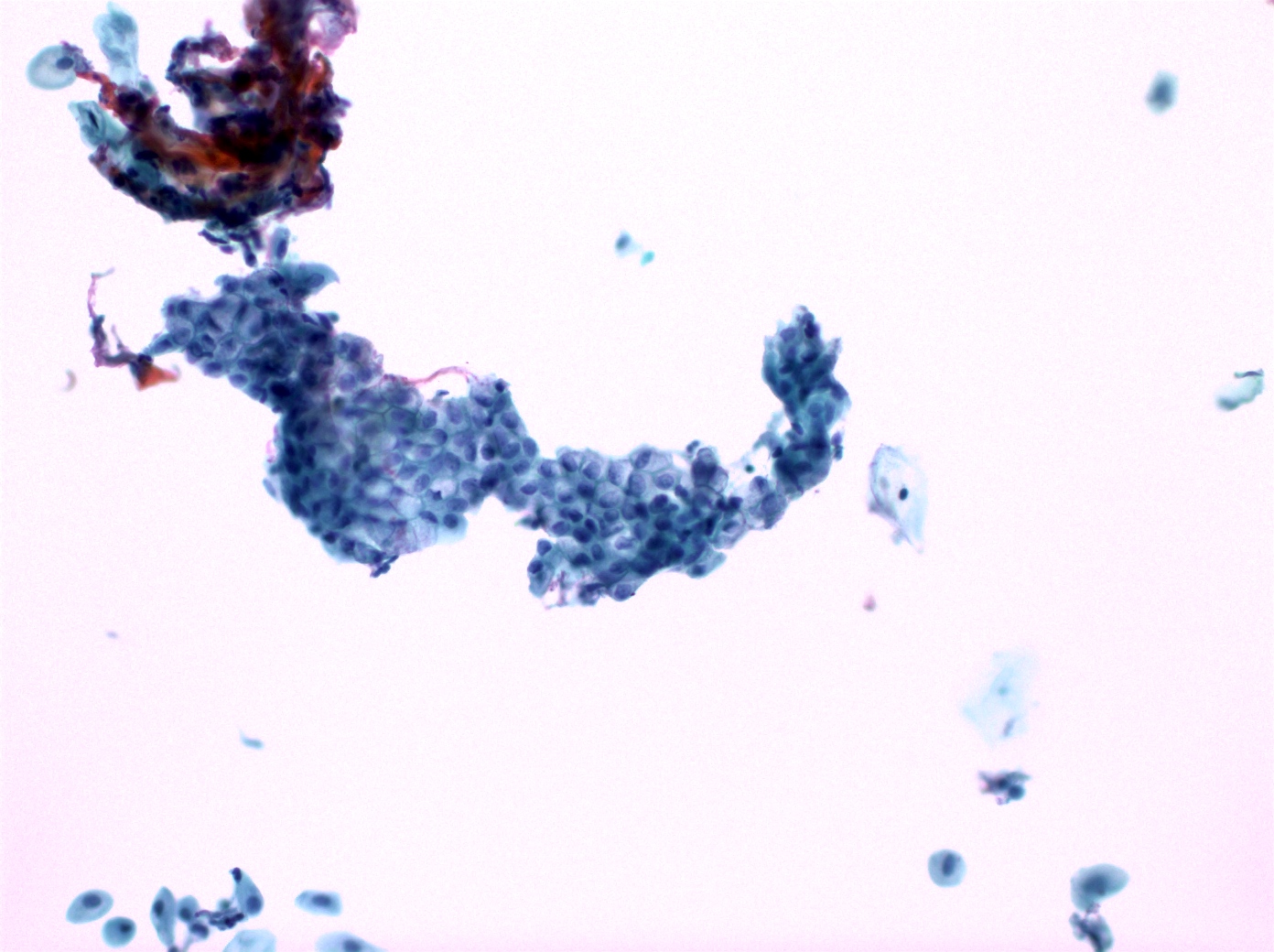
Normal pancreatic acinar cells
High cellularity with cohesive grape-like clusters (acini) singly and in tissue fragments attached to fibrovascular stroma; single cells are few
Round, eccentric nuclei with fine chromatin and single small nucleolus, and abundant bichromatic and granular cytoplasm
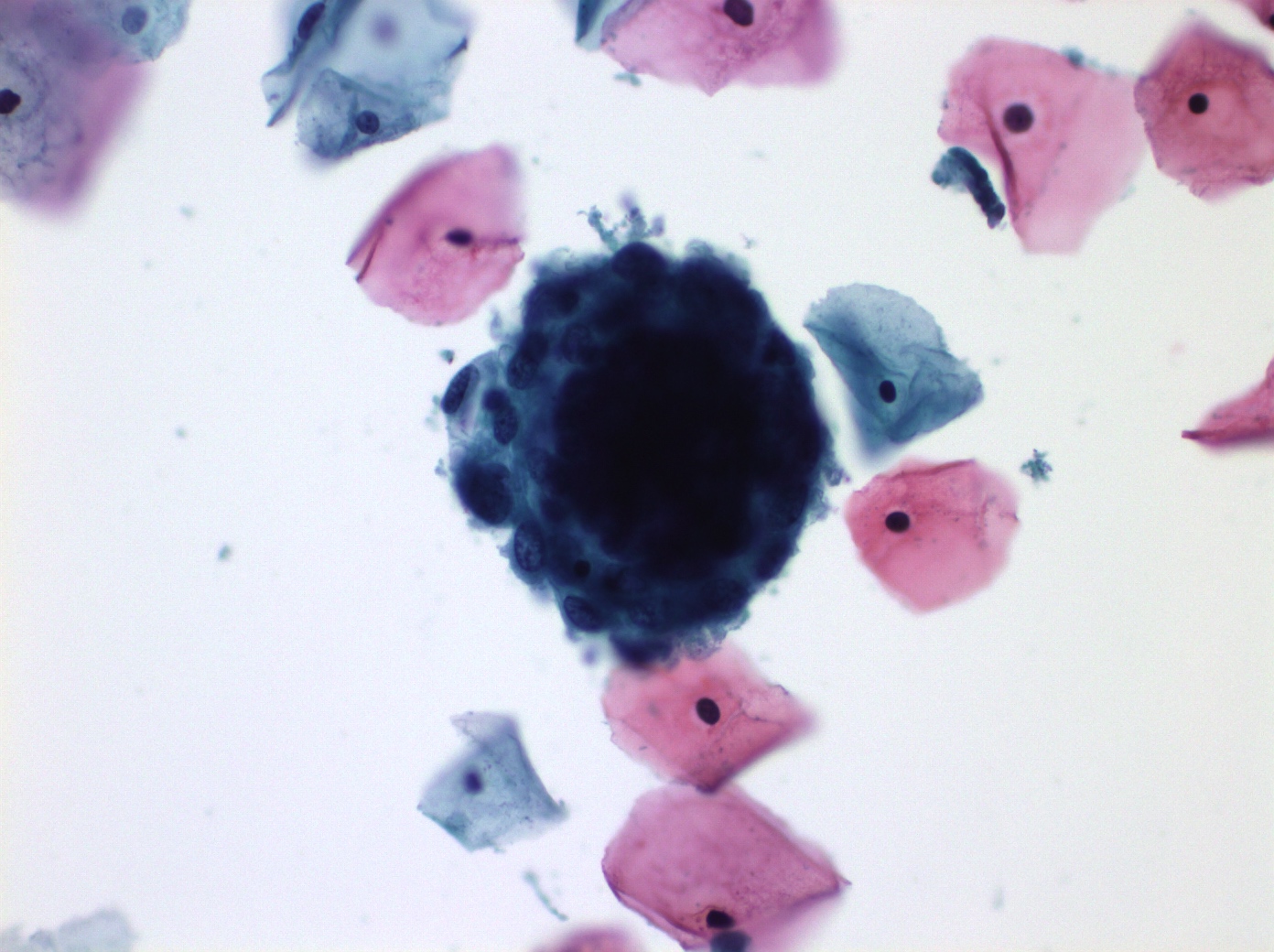
Normal pancreatic ductal cells
Flat, cohesive sheets with even nuclear spacing
Round to oval nuclei, inconspicuous nucleoli and fine chromatin, and non-mucinous cytoplasm
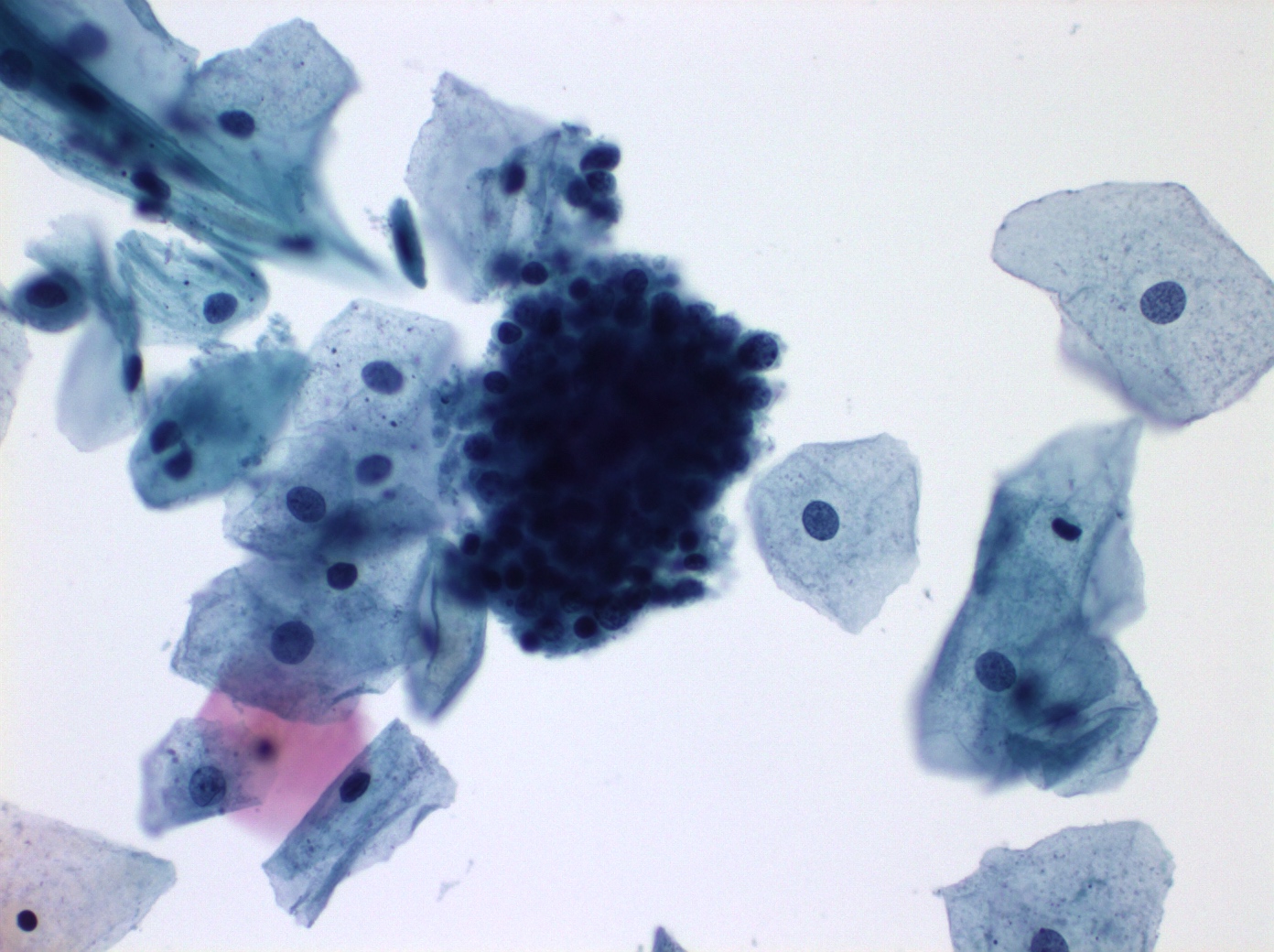
Duodenal epithelium
Flat, monolayered honeycomb sheets
Non-mucinous columnar glandular cells with a brush border
Sporadic goblet cells
Lymphocytes ( sesame seeds ) within epithelium
Gastric epithelium
Small sheets, strips, single cells, and pits, with chief cells and parietal cells
Visible cytoplasmic mucin in the upper third of the cytoplasmic compartment (mucin cup) of foveolar cells at the edge of sheets
Naked nuclei with grooves
Mesothelium
2D sheets, with or without intercellular windows
Round to oval central nuclei, conspicuous nucleoli, and moderate cytoplasm
Hepatocytes
Polygonal with round to oval and usually central nuclei, prominent single nucleoli, and abundant cytoplasm, often with bile pigment and iron
Kidney
Benign glandular cells representing renal tubular cells and intact glomeruli
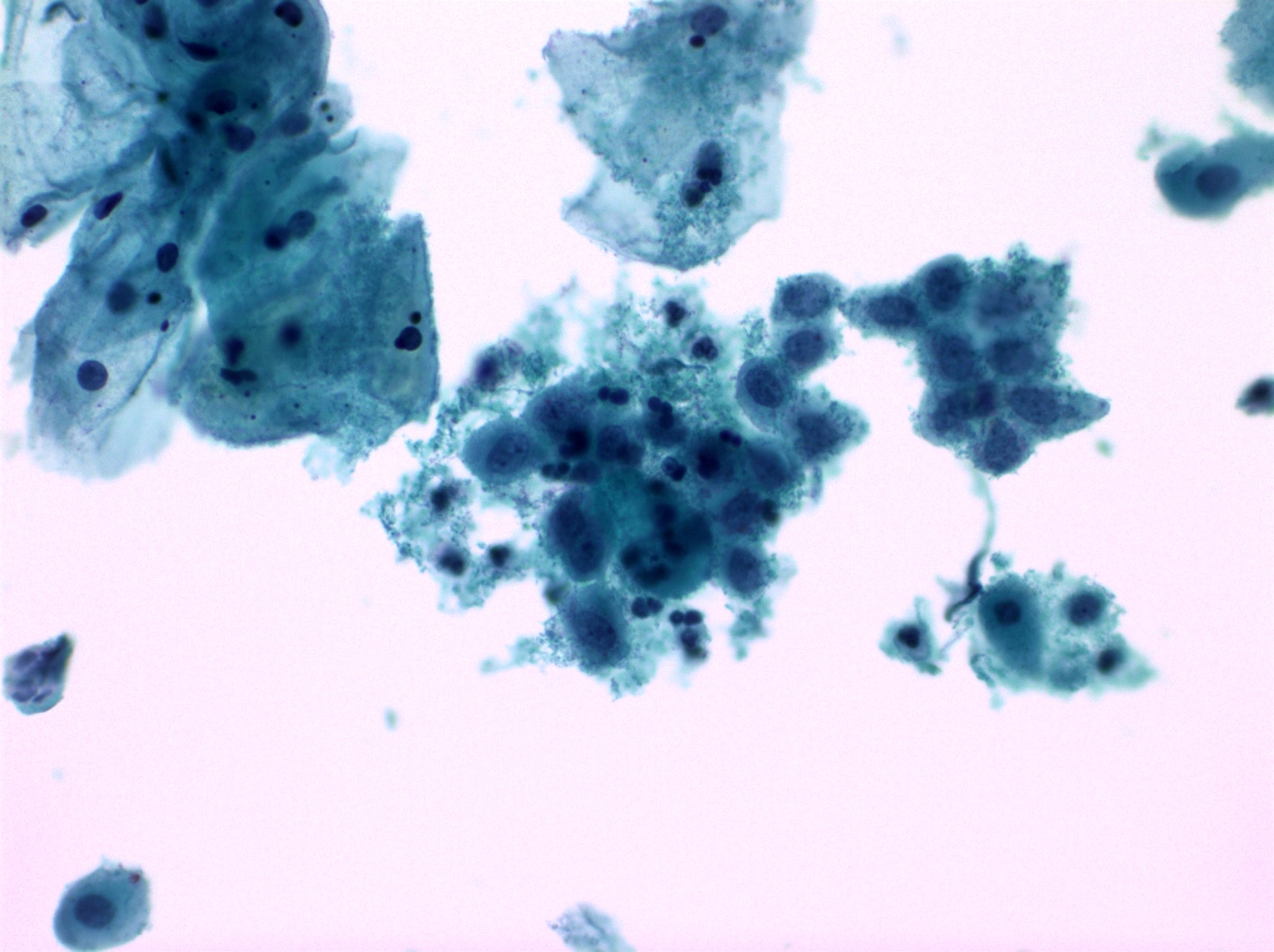
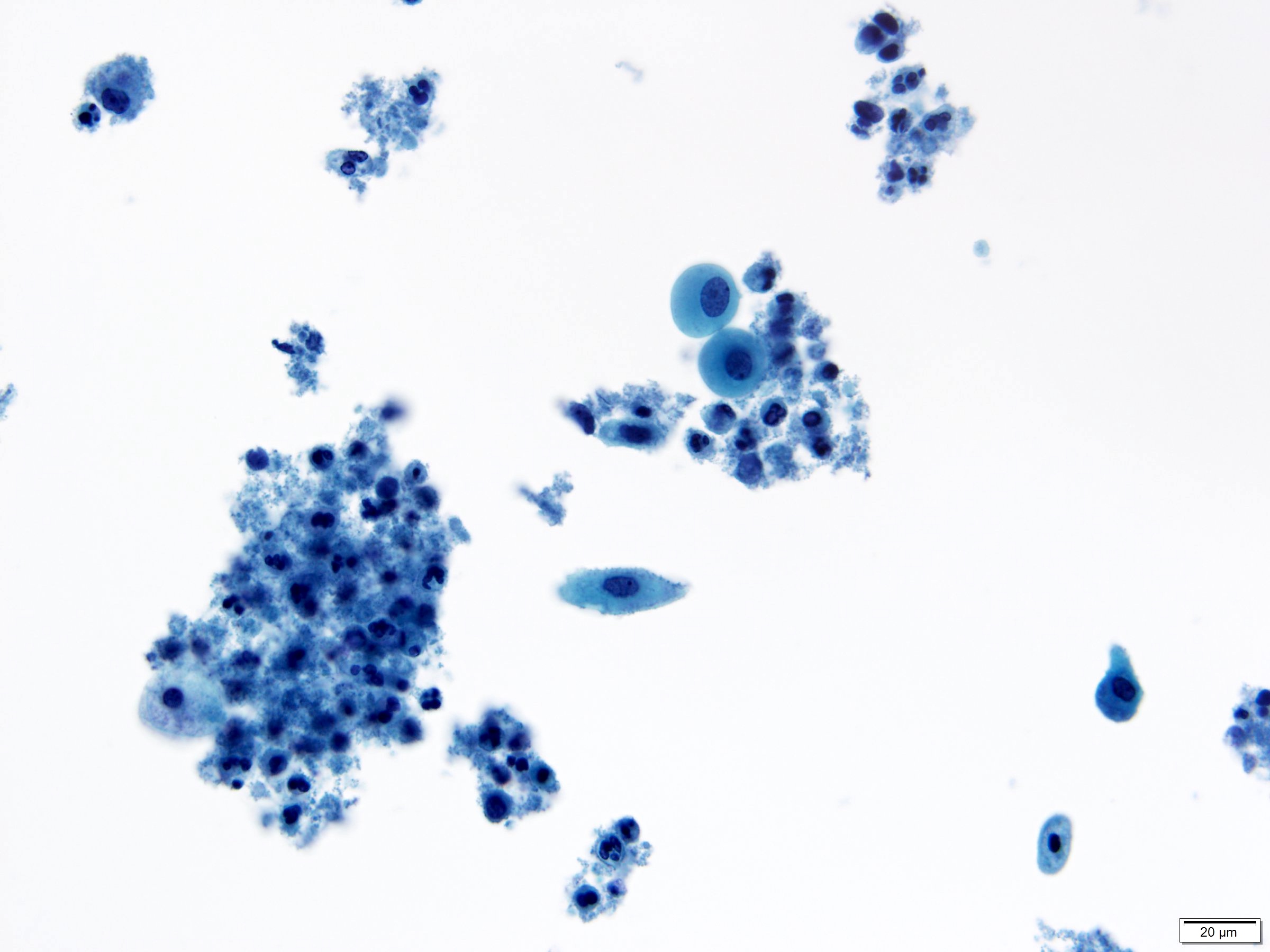
Acute pancreatitis
Cytology predominantly neutrophils
degenerated cells, fat necrosis, foamy histiocytes
calcs esp in necrotizing type
atypia of ductal cells, moderate to severe
enlarged, irregular nuclei
conspicuous nucleoli
Cholangitis
Cohesive sheets of variable size with hyperplastic changes
Mild anisonucleosis (2 3 variation)
Single epithelial cells of normal size and shape
Columnar cells with poorly defined cell cell borders with or without dense cytoplasm indicating metaplasia
Nuclei are enlarged with slight hyperchromasia; smooth and round nuclear membranes; and small, centrally located nucleoli
Inflammatory background
Key cytopathological findings that suggest cholangiocarcinoma over cholangitis include 3D tissue fragments, nuclear pleomorphism, high N:C ratio (> 0.5), nuclear membrane irregularity, hypercellularity, atypical single cells, hyperchromasia, intracytoplasmic mucous vacuoles, prominent nucleoli, nuclear moulding, and a cell population showing two distinct cell types
The difference between cholangitis and BilIN is more subtle. BilIN is typically diagnosed incidentally in surgically resected specimens of longstanding chronic cholangiopathy and does not cause biliary obstruction.
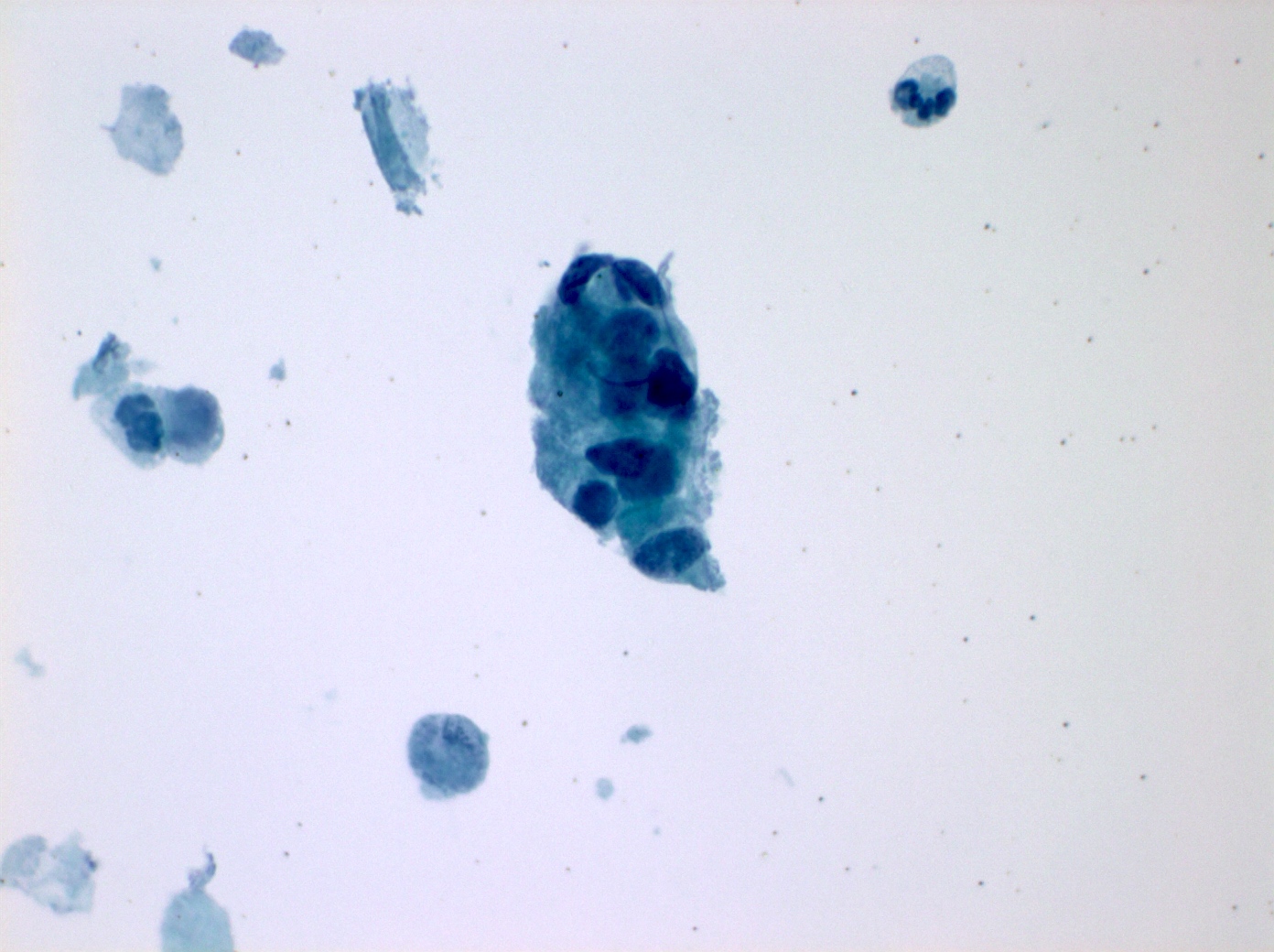
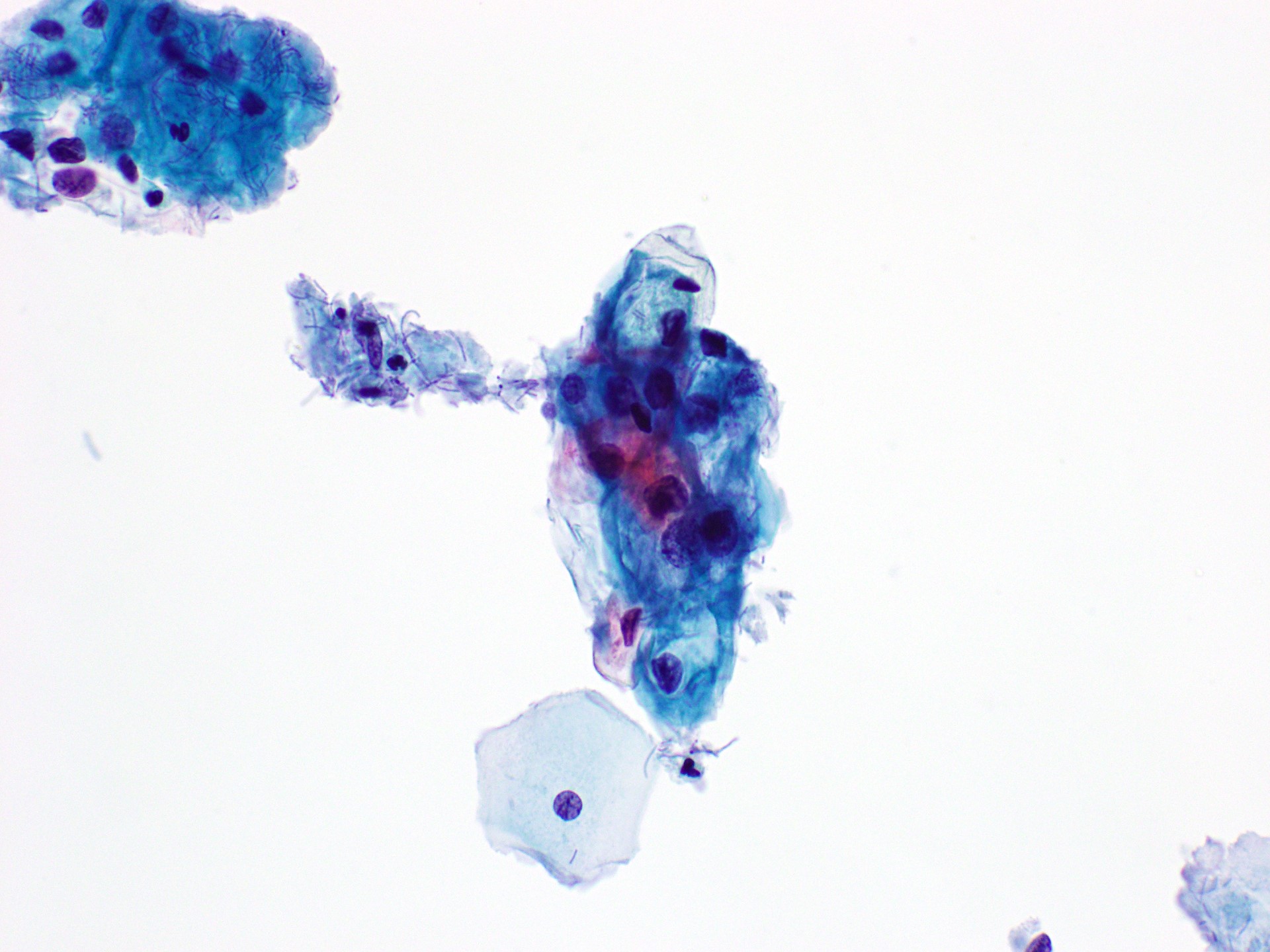
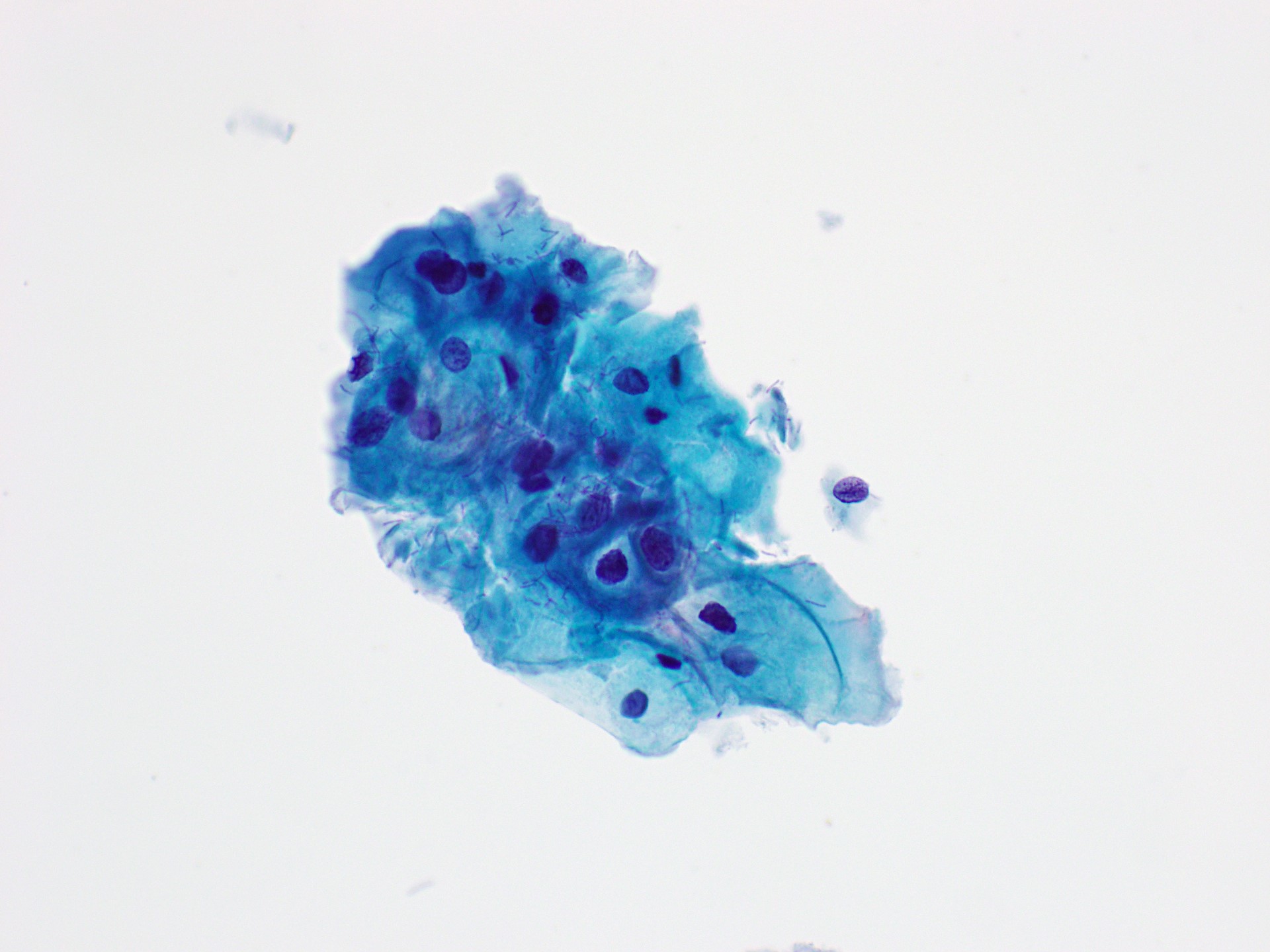
Chronic pancreatitis
Cytology cells hypocellular and bloody
benign acini splayed apart by fibrosis
Nuclei enlarged, crowded, slight anisonucleosis
prominent nucleoli
other myofibroblasts may be present
vesicular nuclei
prominent nucleoli
islet cells may be present
back fat necrosis, debris, and calcifications
The major differential diagnosis of localized CP is pancreatic ductal adenocarcinoma. Reactive ductal cells can show significant cytopathological atypia in response to CP, which overlaps with well-differentiated pancreatic ductal adenocarcinoma { 27926365 }. Extensive high-grade pancreatic intraepithelial neoplasia may be present in CP and can pose a diagnostic challenge on cytopathology { 25410732 ; 20730891 ; 27889759 }. Cytopathological atypia seen in CP is almost always focal and limited to rare groups of ductal cells. Features diagnostic of pancreatic ductal adenocarcinoma, such as single atypical cells, significant anisonucleosis > 4:1 in the same tissue fragment, nuclear membrane irregularity, and prominent macronucleoli, are rarely seen in CP { 12589645 }.
Islets of Langerhans may remain even in the late stages of CP. The loss of acinar tissue can lead to aggregation of islets, which can result in islet cells being prominent on FNAB, posing a diagnostic pitfall for pancreatic neuroendocrine tumour (PanNET) { 25410732 ; 21737075 }. The diagnosis of PanNET should be applied cautiously when only a small number of the islet cells are present in a background of CP. Correlation with imaging is helpful because PanNETs are clearly visible, round, enhancing mass lesions { 21548125 }. Spindle cells in fibrotic tissue may show plump vesicular nuclei, prominent nucleoli, and occasional mitoses, mimicking a spindle cell neoplasm.
Chronic Pancreatitis & Reactive Ductal Atypia
cytology cellularity low, low NC, flat cohesive sheets
nuclei enlarged, no significant variation in size
nuclei round with smooth nuclear membrane
nucleoli prominent but not macronucleoli
background inflm, fat necrosis, Ca⁺⁺
cellular stromal fragments with crush artifact (autoimmune)
abset to rare atypia & mitosis
IHC retained SMAD4/DPC4 & p16 (CDKN2A)
wt p53
note see Pancreatitis
acute pancreatitis does not form a mass so not FNA d
PSC, PBC, stents, & stones have a higher threshold[2]
Groove/paraduodenal pancreatitis
Autoimmune and IgG4-related pancreatitis
Lymphoepithelial Cyst
radio unilocular or multilocular, may be solid form debris
cytology cellularity variable
anucleate squames, abundant keratin debris
mature superficial squames
lymphocytes cholesterol crystals
note cyst fluid CEA very high
Pseudocyst
Cytology dirty proteinaceous background, often with necrosis
Mixed inflammation dominated by lymphocytes and histiocytes
Hemosiderin-laden macrophages
Red blood cells, yellow-brown haematoidin-like pigment
cholesterol crystals, calcified debris, and cell debris
No epithelial component except for gastrointestinal contaminants
Rarely, fragments of granulation tissue may be present
note sx acute pancreatitis should be present
Splenule (accessory spleen)
Cytology Heterogeneous population of predominantly small lymphocytes
lesser number of larger lymphoid cells
Lymphoid cells form cohesive tissue fragments
Small sinusoidal vascular structures with admixed lymphocytes
Large platelet aggregates
No tingible-body macrophages
Serous cystadenoma
epid 2% pancreatic tumors
microcystic in older F; oligocystic in kids
radio spongy appearance of small cysts
central stellate scar
cytology cellularity sparse, in sheets or loose clusters
nuclei round, little to no atypia
chromatin evenly distributed
nucleolus inconspicuous
cytoplasm clear, finely vacuolated/granular
cell shape cuboidal, cell borders indistinct
backgrond clean or bloody
IHC (+) Glut-1 & α-inhibin
PAS+ PASD- (cytoplasmic glycogen)
mol VHL
note see Serous Cystadenoma
cyst fluid low amylase & low CEA (5 to 192)
media WSI Pap HE inhibin Glut1[3]
Schwannoma
Lymphangioma
epid F >> M, wide age range
site distal pancreas
radio well-circumscribed, thin-walled, uni/multilocular
cytology non-mucinous cyst fluid[8], proteinaceous
scattered histiocytes, mature lymphocytes, no atypia
note see lymphangioma
MRI useful for excluding ductal connection
media WSI
Other rare benign neoplasms
Atypical
Loss of architectural polarity
Minor nuclear crowding
Mildly alteratered honeycomb
No true nuclear moulding
Near-normal N:C ratio
Slight nuclear membrane irregularity without marked clefting
Parachromatin clearing without other features of adenocarcinoma
Small nucleoli without macronucleoli
Minor anisonucleosis (2:1)
Clean background without necrosis, which might not be important in BDB because necrosis is not helpful in identifying malignancy in BDB {
Pancreaticobiliary neoplasm (low & high risk)
Pancreatic intraepithelial neoplasia
Low or high risk
Biliary intraepithelial neoplasia
WHO Low or high risk
Pancreatic intraductal papillary mucinous neoplasm
WHO Low or high risk
cytology cellularity low
extracellular mucin variable
note see IPMN
mucinous cyst fluid thick
Intraductal papillary neoplasm of the bile duct
WHO Low or high risk
Mucinous cystic neoplasm
WHO Low or high risk
epid 5% pancreatic neoplasms
radio one or more locules, fine septa
no ductal communication
cytology LG ~gastric contaminant
mod atypia
nuclear stratification (intermediate)
HG cell size small (~12μm enterocyte)
single or in tight clusters
NC high
chromatin hyper or hypochromatic
cytoplasm vacuolated (variable)
background necrosis
malign 3D groups, marked anisonucleosis
nuclear membranes irregular
nucleoli prominent
chromatin w parachromatin clearing
background necrosis
note see Mucinous Cystic Neoplasm
resected irrespective of grade (costly surveillance)
cannot differentiate from IPMN without ovarian stroma
Intraductal oncocytic papillary neoplasm
WHO high risk
Intraductal tubulopapillary neoplasm
WHO high risk
Other WHO low-risk lesions (including spindle cell tumours)
WHO Low risk
Suspicious for malignancy
Note cases scant sampling of a well diff
rare atypical ductal cells
indwelling stents, inflammatory conditions (PBC)
Malignant
Cholangiocarcinoma
Key diagnostic cytopathological features
Loss of honeycomb pattern (drunken honeycomb)
3D architecture
Hypercellularity with two-cell population
Hypochromasia/hyperchromasia
Nuclear pleomorphism
Anisonucleosis (threefold to fourfold variability, or greater, in nuclear size in a single cell group)
Increased N:C ratio (≥ 0.6)
Cytoplasmic mucin
Cellular discohesion with atypical single cells
Prominent nucleoli
Enlarged nuclei
Loss of polarity
Bloody background
Flat nuclei
Cell-in-cell arrangement
Nuclear moulding
Chromatin clumping
Solid Pseudopapillary Neoplasm
cytology cellularity high, solid-cellular pattern
nucleus bean-shaped, grooved, perinuclear vacuoles
nucleolus inconspicuus
cytoplasm finely vacuolated
cell borders indistinct
vascular stalks ependymal rosettes
PASD+ hyaline globules
foam cells & necrotic debris
little pleomorphism or anisonucleosis
IHC (+) β-catenin (nuclear)
IHC (-) keratin
note see Solid Pseudopapillary Neoplasm
media WSI Pap Pap HE β-catenin[11]
Pancreatoblastoma
cytology cells syncytial groups & isolated cells
cytoplasm moderate
squamous morules
stroma primitive spindle cells
occasional heterologous elements
IHC (+) nuclear β-catenin in squamous morules
Neuroendocrine &/or acinar diff
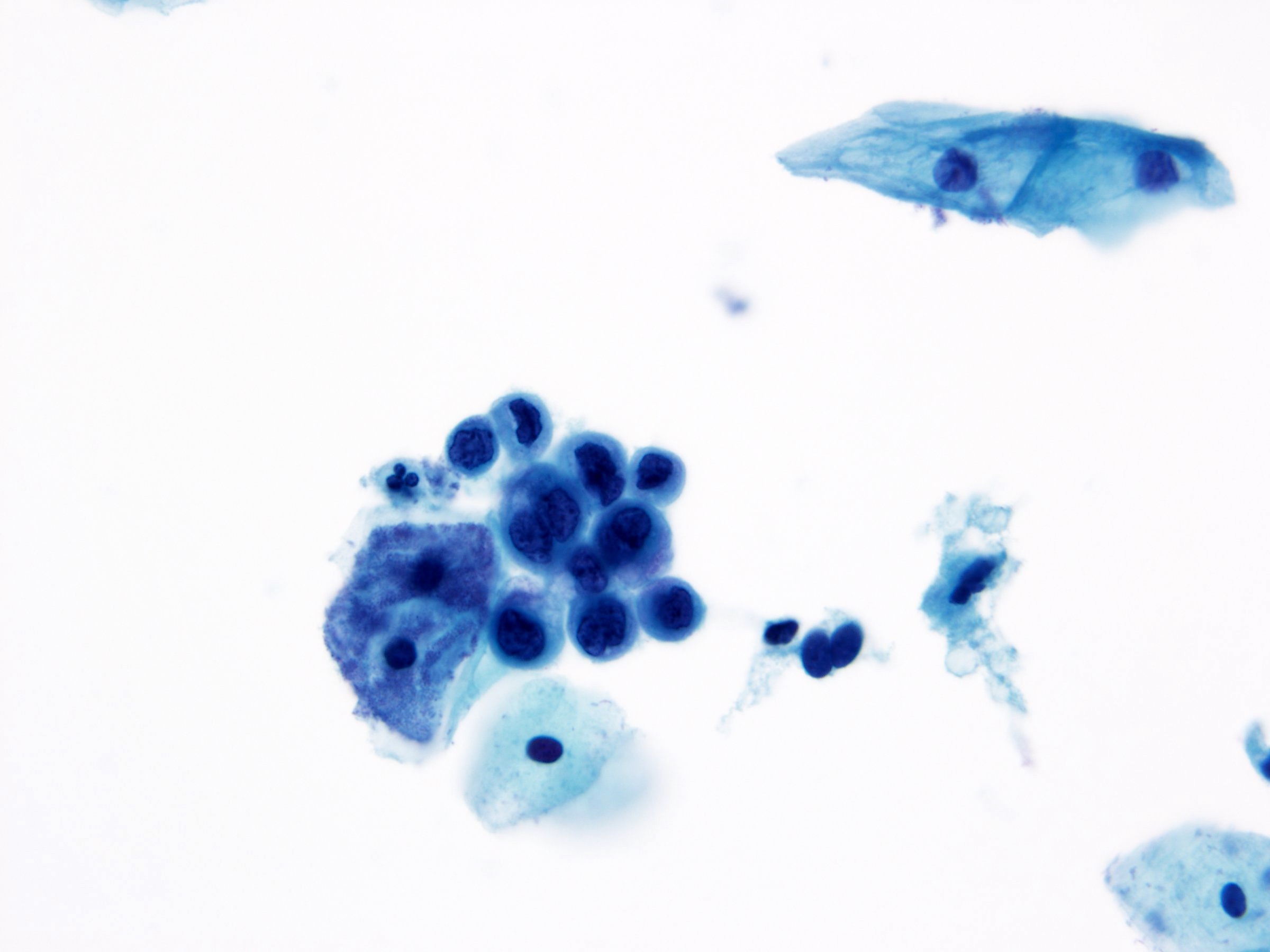
Pancreatic Ductal Adenocarcinoma
cytology cells cellularity moderate to high
loss of polarity in sheets (drunken honeycomb)
nuclei hypochromatic with parachromatin clearing
nucleoli may be present and prominent
enlarged nuclei, irregular contours, 4:1 anisonucleosis
cytoplasm mucinous, sometimes finely vacuolated and lacy
may have a deceptively low N:C ratio
background clean background if well diff
necrotic background if high-grade
IHC SMAD4 loss, p16 loss, p53 mutant
Mol KRAS, SMAD4, CDKN2A, TP53
Note see Pancreatic Ductal Adenocarcinoma
double duct sign[12]
well-diff & foamy gland variant[13]
adenosquamous carcinoma variant
undifferentiated (anaplastic) carcinoma variant
undifferentiated carcinoma with OLGC variant
Pancreatic Neuroendocrine Tumor
cytology cells highly cellular specimen, loosely cohesive
epithelioid or plasmacytoid
nuclei round to oval, salt-and-pepper chromatin
Smooth, dense nuclear membranes
Nucleoli may be present, occasionally prominent
cytoplasm dense, often eccentric, abundant, and granular
occasionally minimal
background clean, without necrosis
IHC (+) synaptophysin, INSM1
mol mutations in MEN1, ATRX, DAXX
mTOR alterations less common (PTEN, PI3KCA, TSC2)
DDx SPN lacks coarse chr, nuclear grooves present
acinar cell ca prominent nucleoli
granular cytoplasm
adenocarcinoma necrosis, desmoplastic stroma
PanNEC extensive necrosis
high mitotic activity
Pancreatic Neuroendocrine Carcinoma
aka PanNEC
Small cell neuroendocrine carcinoma
cytology nuclei angulated, pleomorphic
coarse chromatin
nucleoli inconspicuous
cytoplasm minimal, imperceptible
background necrosis, apoptotic bodies
mol RB1, TP53 mutations
Large cell neuroendocrine carcinoma
cyto nuclei markedly enlarged
coarsely stippled chromatin
nucleoli prominent
cytoplasm moderate to abundant, eosinophilic
IHC (+) synaptophysin, INSM1
mol RB1, TP53 mutations
Acinar cell Carcinoma
cytology cells high cellularity
many isolated cells, loose cell aggregates
nuclei enlarged, eccentric, round, & smooth
nucleolus prominent
cytoplasm granular cytoplasm
negative image of zymogen granules (Giemsa)
background naked tumor nuclei
loose granules in the background
IHC (+) BCL10, trypsin, synaptophysin (focal)
Mol APC, CTNNB1, TP53, BRAF
note see Acinar Cell Carcinoma
─ Cyto ─ GYN
Media automation pathoutlines
Media preparations pathoutlines
Adequacy
Note age, LMP, appropriate labelling
5K well-preserved squames on LBP
ie ThinPrep, SurePath
8-12K on conventional smears
Fewer cells in certain settings
post-menopause/atrophic
vaginal specimen/post-therapy
Transformation zone preferred, not required
Unsat if 75% obscured (blood, inflm, drying artifacts)
media video
Benign GYN Cytology
Media normal and nonneoplastic findings pathoutlines
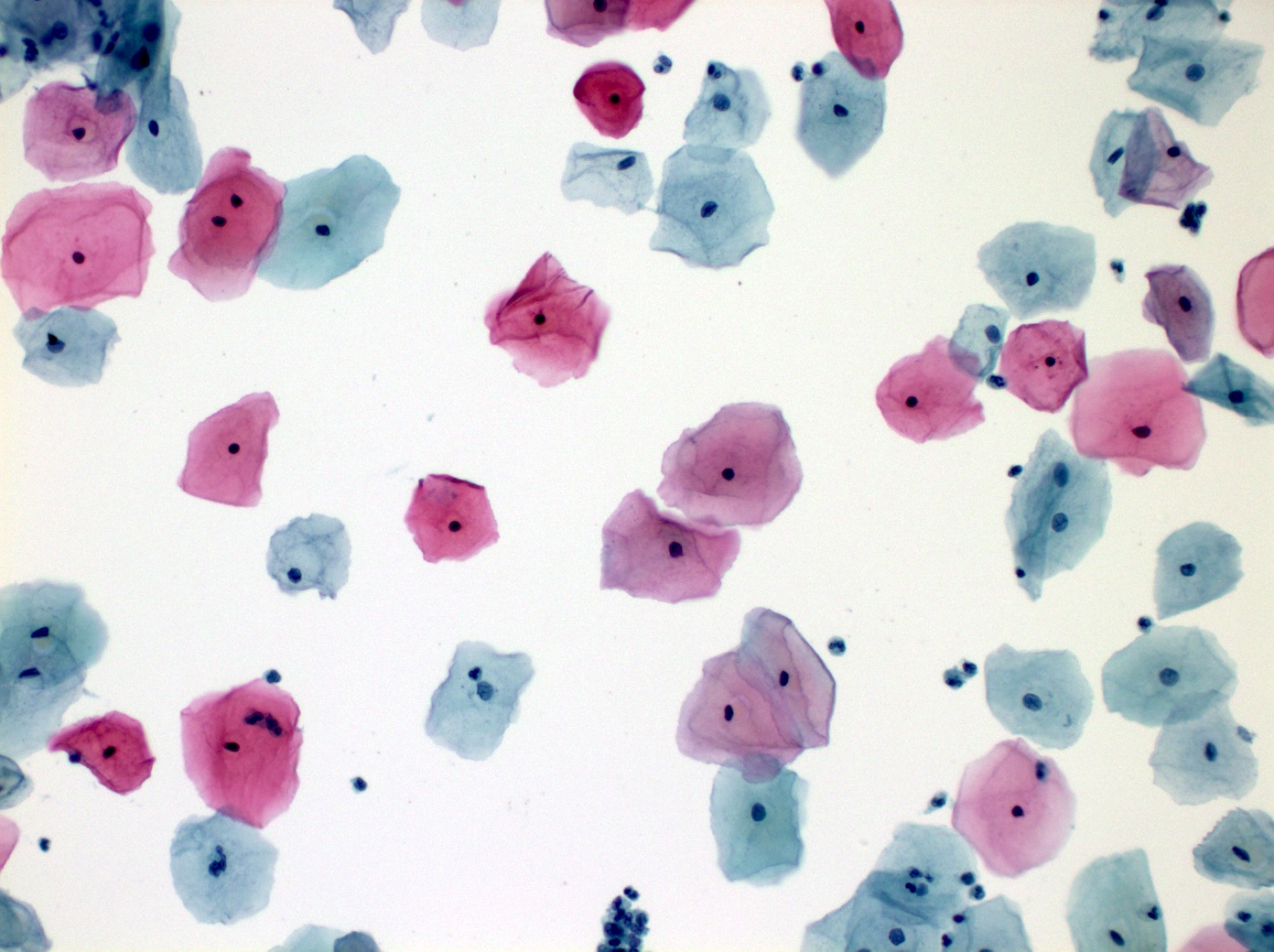
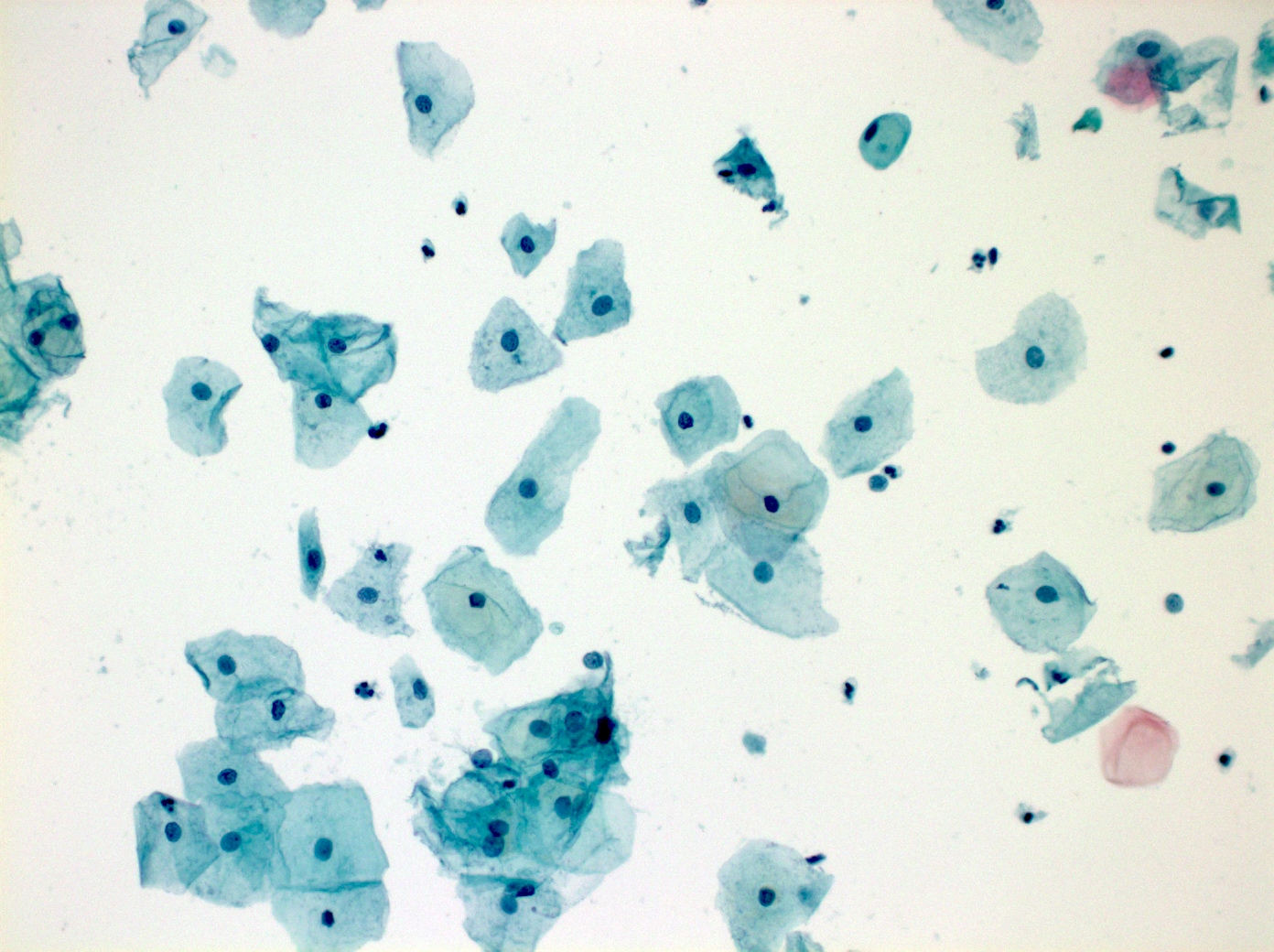
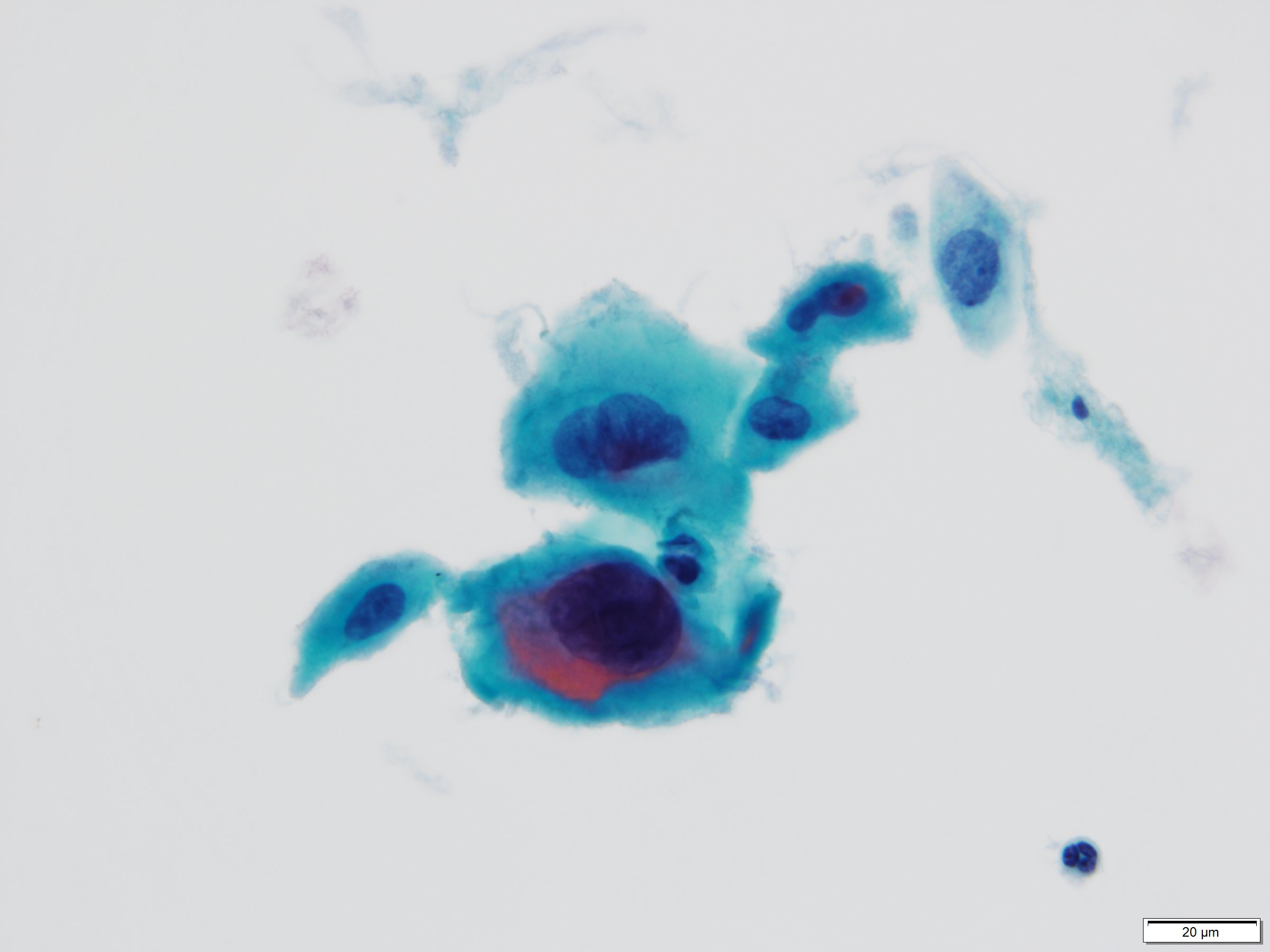
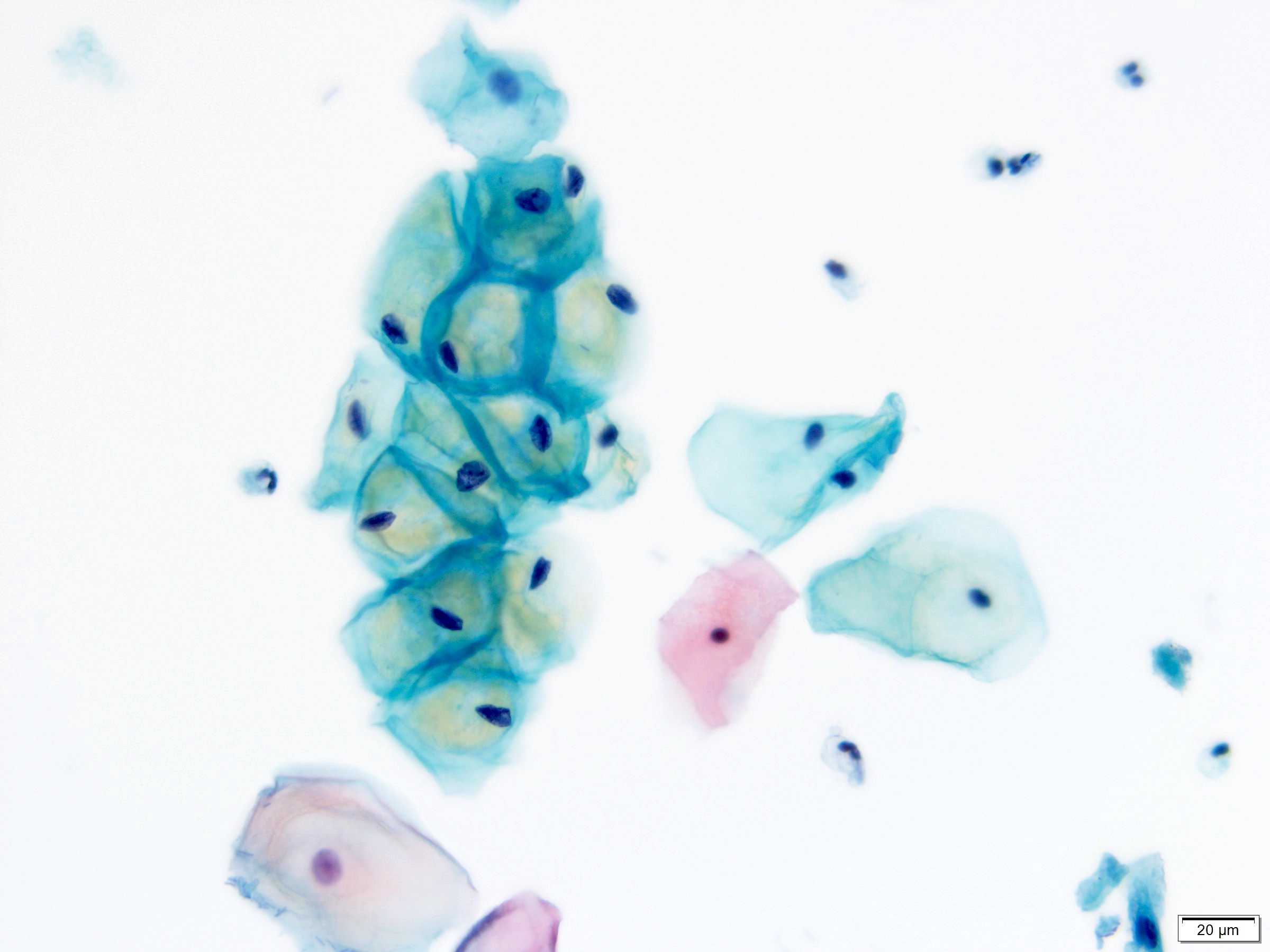
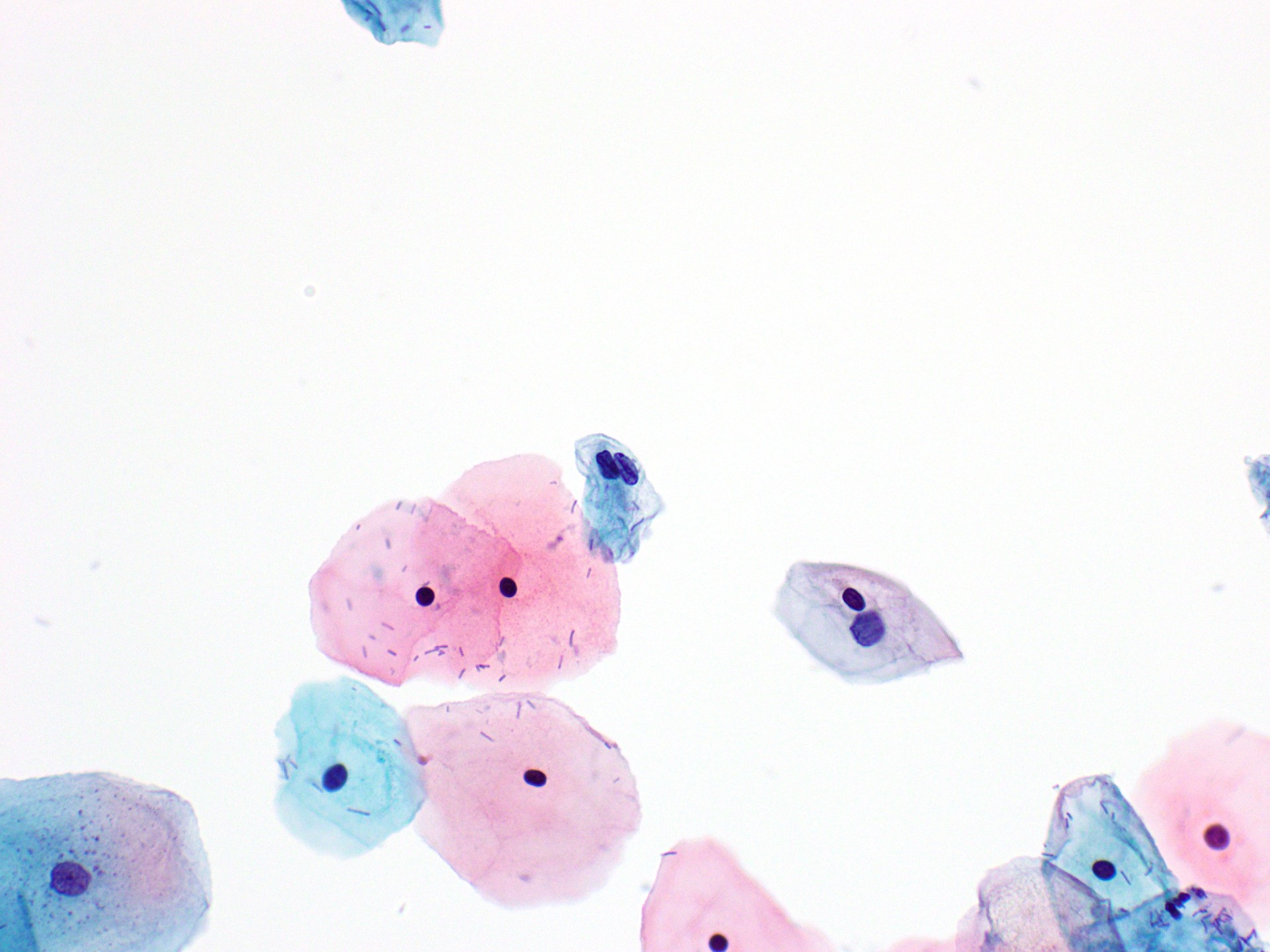
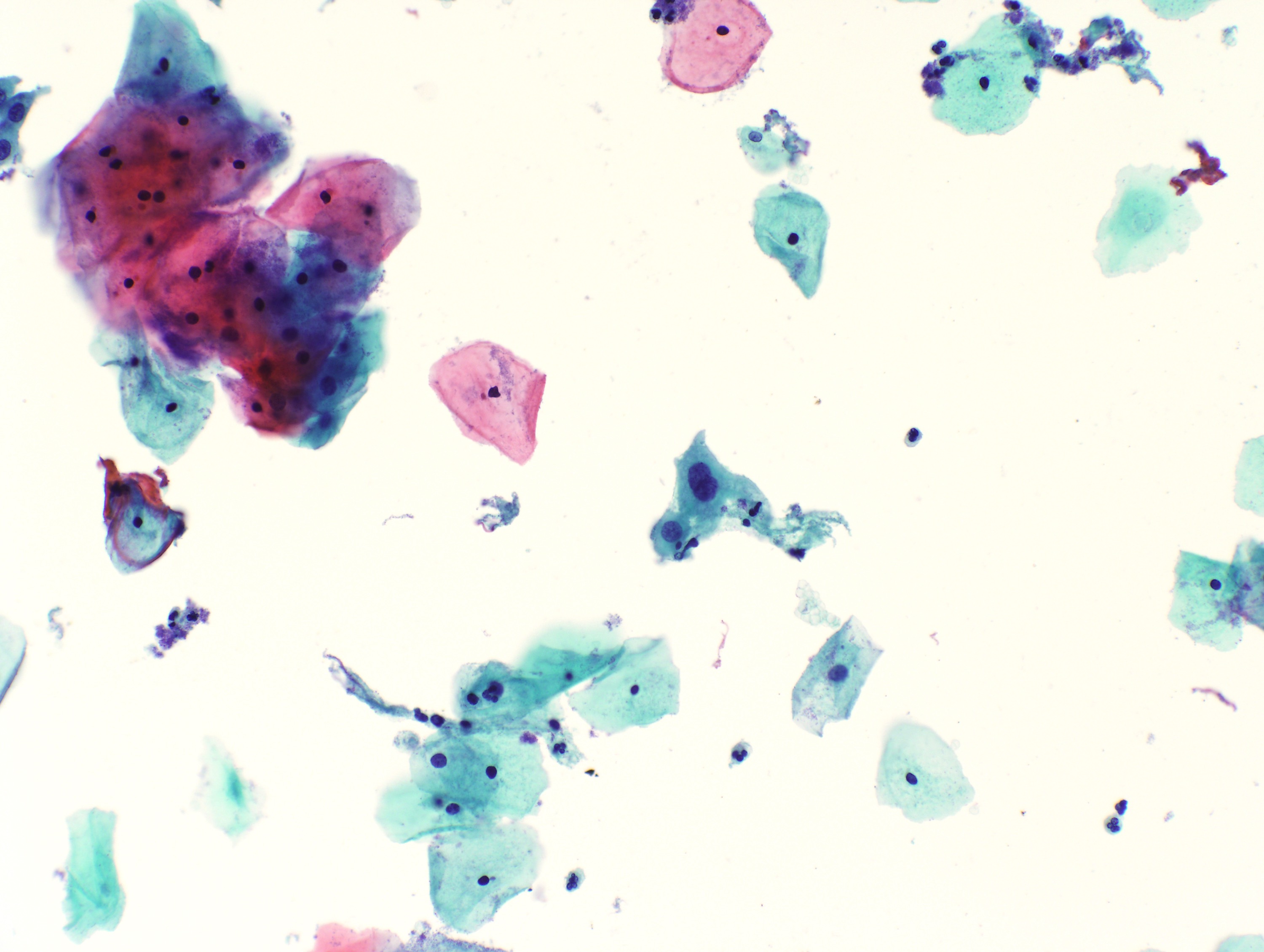
Squamous cells
media WSI collection
Superficial
Micro pink cyto, dense nucleus
note proliferative phase, inhbited by progesterone
media Pap
{kind=link}
Intermediate
Micro blue abundant cytoplasm
granular chromatin, nuclear groove
note secretory phase
{kind=link}
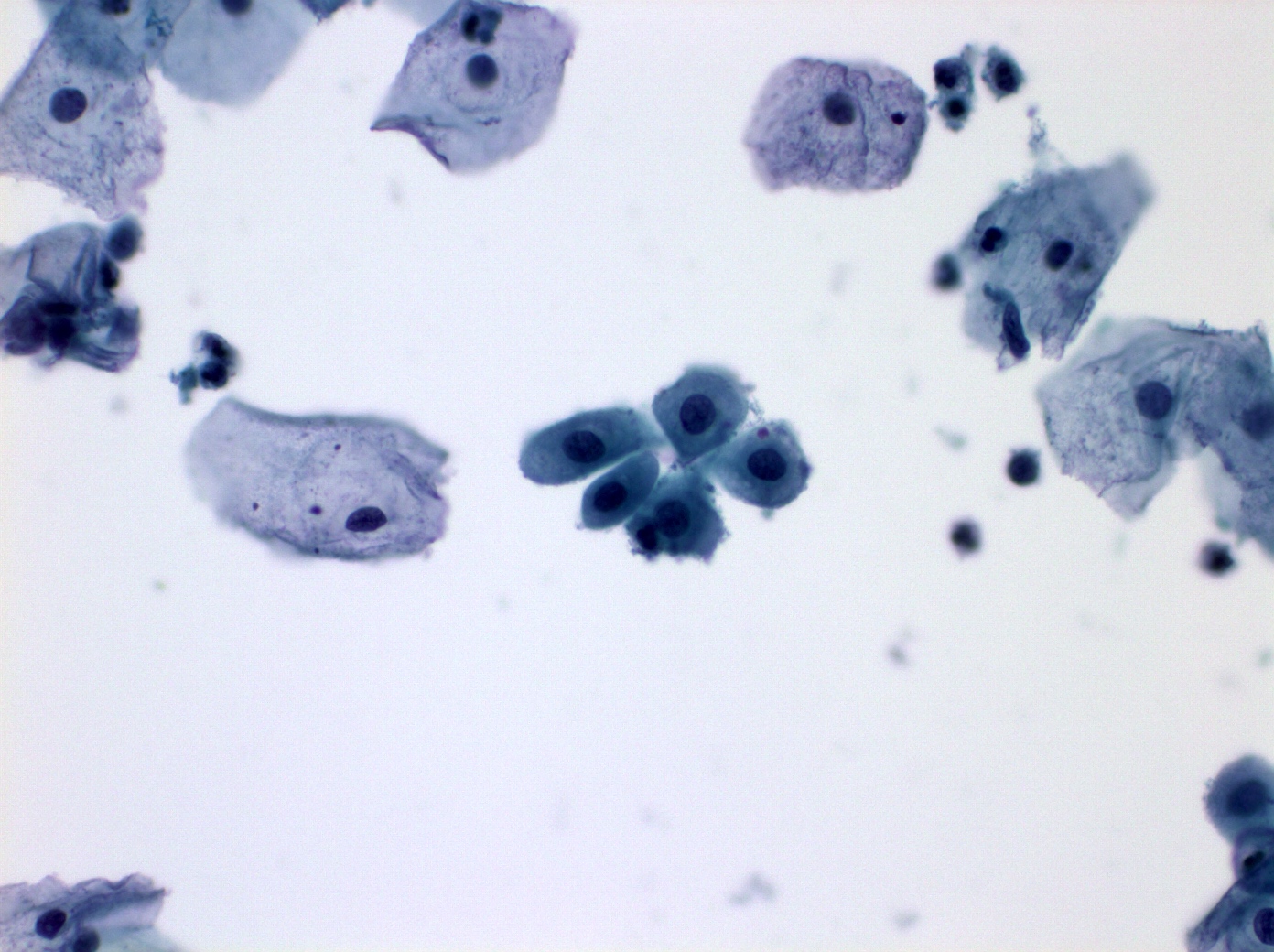
Parabasal
Micro nuclear groove, abundant cytoplasm
granular chromatin
note postmenopause or htx
{kind=link}
Glandular cells
media WSI collection
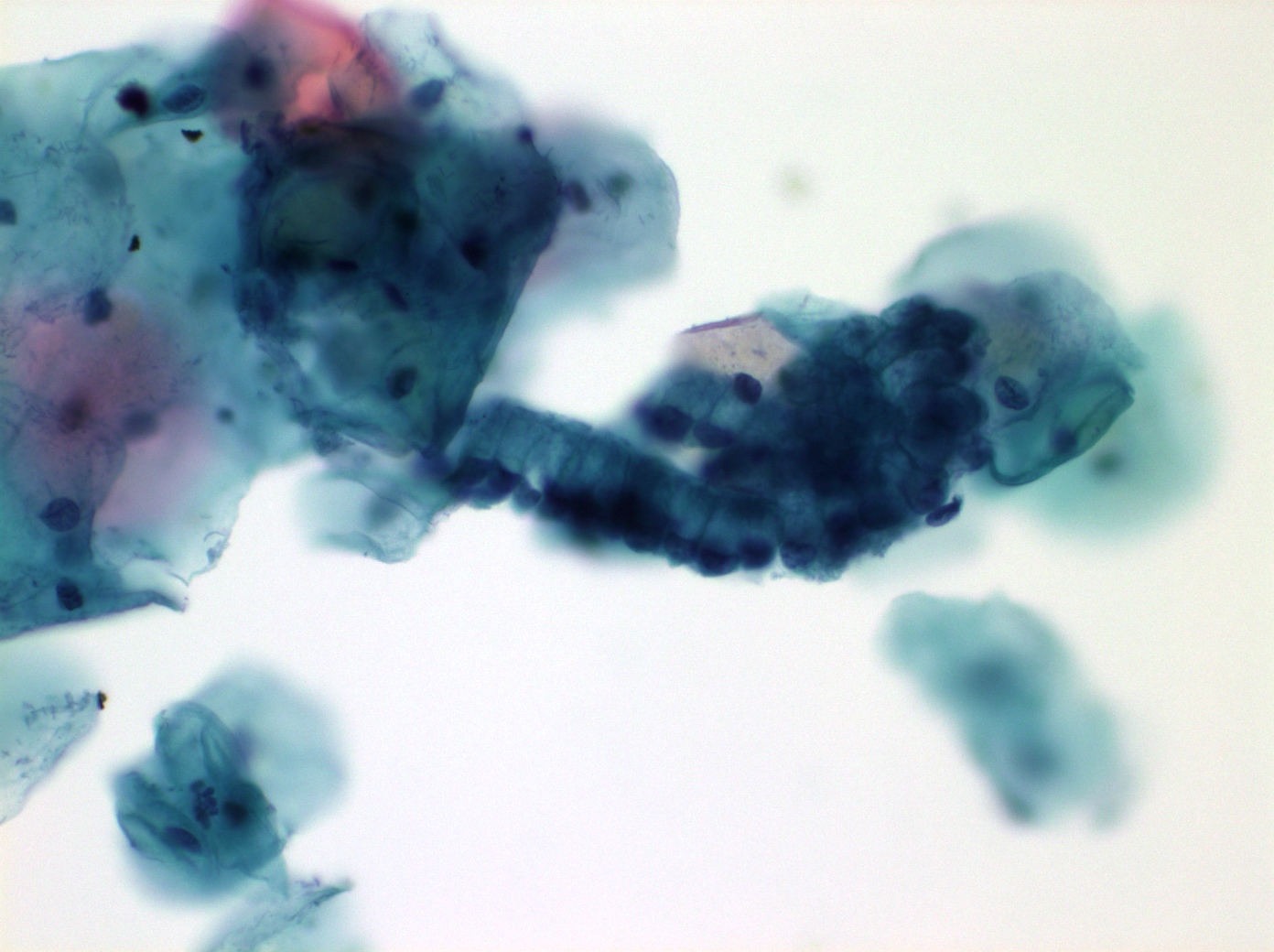
Endocervical glandular cells
Micro size variable but > IMC
Chromatin finely granular, evenly distributed
Nucleoli small
Ciliated cells cilia, polarized
terminal bar
Secretory cells non-ciliated, polarized
honeycomb/picket fence
{kind=link}
{kind=link}
atlas[23] atlas[24] atlas[25] atlas[26]
Endometrial glandular cells
Micro Chromatin dense, heterogeneous
Nucleoli not prominent, except on LBP
Cytoplasm scant, may be dense or vacuolated
Smaller than endocervical, higher NC, size ~IMC or less
Apoptotic debris due to degenerative changes
single or aggregate, spontaneous exfoliated
exodus ball w outer glandular epithelium (pap)
{kind=link}
{kind=link}
{kind=link}
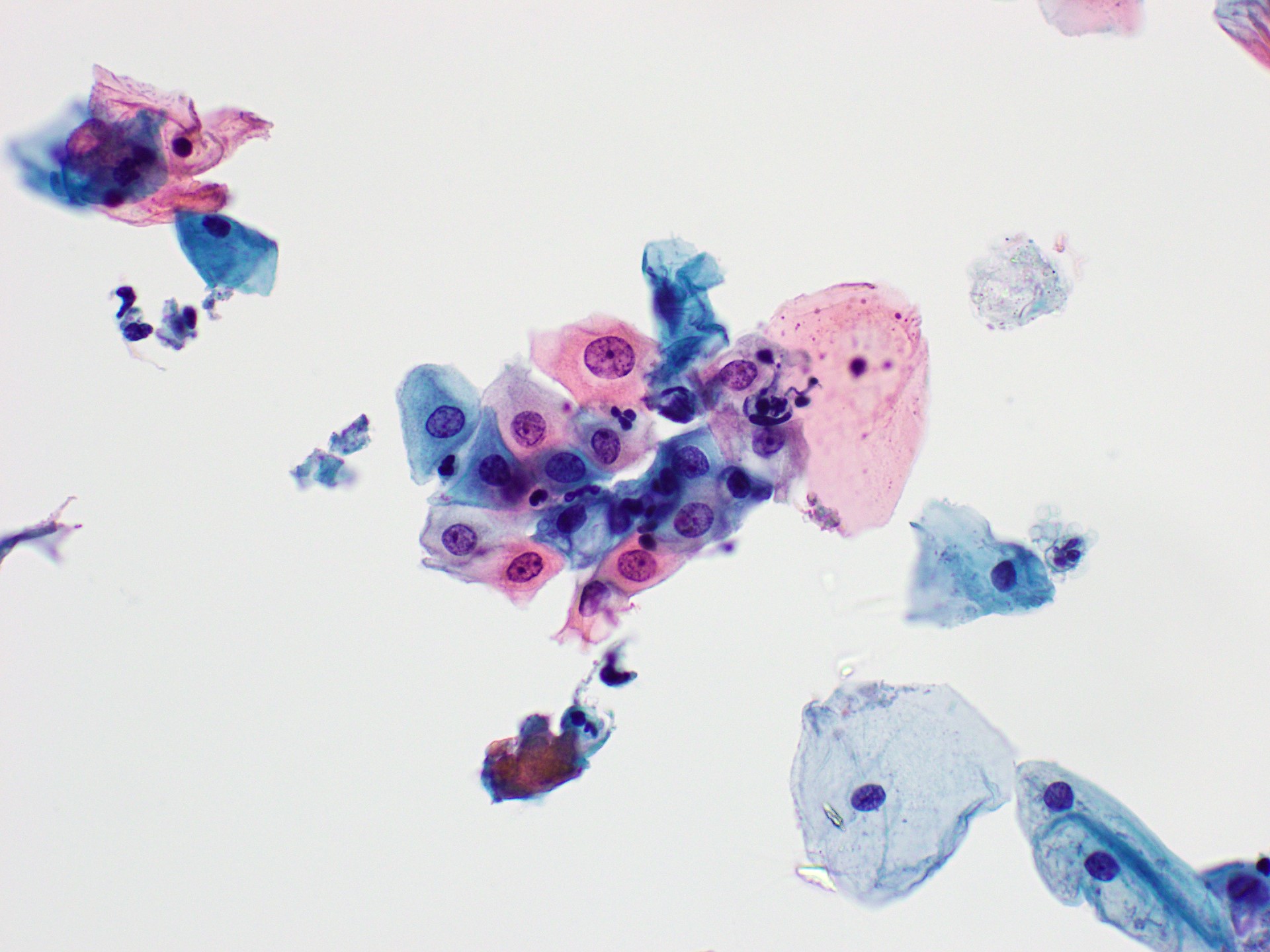
Benign Reactions
media WSI collection
Reactive
Micro nuc enlargement, non-overlapping
Multinucleate, smooth contours, chr uniform
Hyperchr and nucleoli common
Cytoplasmic boundaries well defined
School of fish
{kind=link}
Repair
Micro cohesive, flat sheets, streaming appearance
large nuc w size variation, pale chr, mitoses
large nucleolus, can be mishapen
Metaplasic Squamous cells
Micro parabasal-like to intermediate cell-like
smooth nuclear contour
{kind=link}
{kind=link}
{kind=link}
Tubal metaplasia
Micro Terminal bar, cilia in glandular groups
Often high NC, vacuolated
Media WSI
{kind=link}
Atrophy
Micro monolayer of parabasal-like cells
Nuclei polarized and overlapping
Inc NC, evenly distributed chr, even contours
Background diathesis common[38]
{kind=link}
IUD effect
Micro vacuolated &/or small dark cells w scant cyto
Keratinization
Media pap
{kind=link}
Radiation
Micro nl nc, big cells
{kind=link}
Contaminants and miscellaneous
media WSI collection
Organisms
media WSI collection
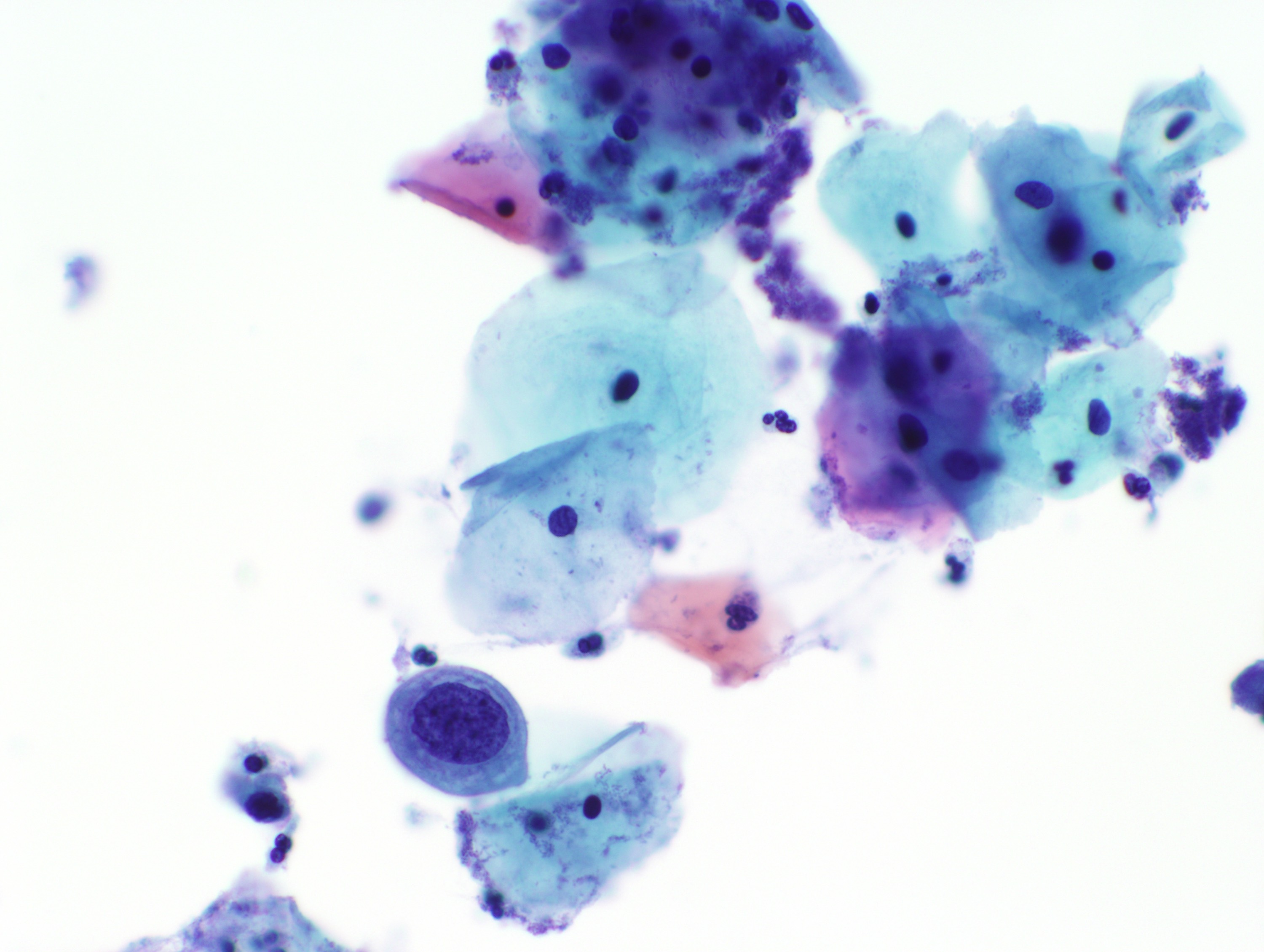
HSV
Micro molding nuclei, marginated chr
ground glass nuc
eosinophlic intranuclear inclusion
CMV
Micro mononuclear large cells
basophilic intranuclear inclusion
smaller granular cytoplasmic inclusions
media pathoutlines
Actinomyces
Epid Actinomyces Israelli is mc subtype
Etio long term IUD use (esp copper)
Pessaries
NF of mouth, bowel, and gyn
Micro cotton ball clumps of filamentous bacteria
media pathoutlines
Trichomonas
Epid mc non-viral STD in USA
Micro pear-shaped, pale, eccentric nuclei
red cytoplasmic granules; Trich Picnics
note diagnose by NAAT
often accompanied by Leptothrix
media pathoutlines
Candida
Micro Psedohyphae & true hyphae
Shish-kebabs[46] with spaghetti & meatballs[47]
Media WSI
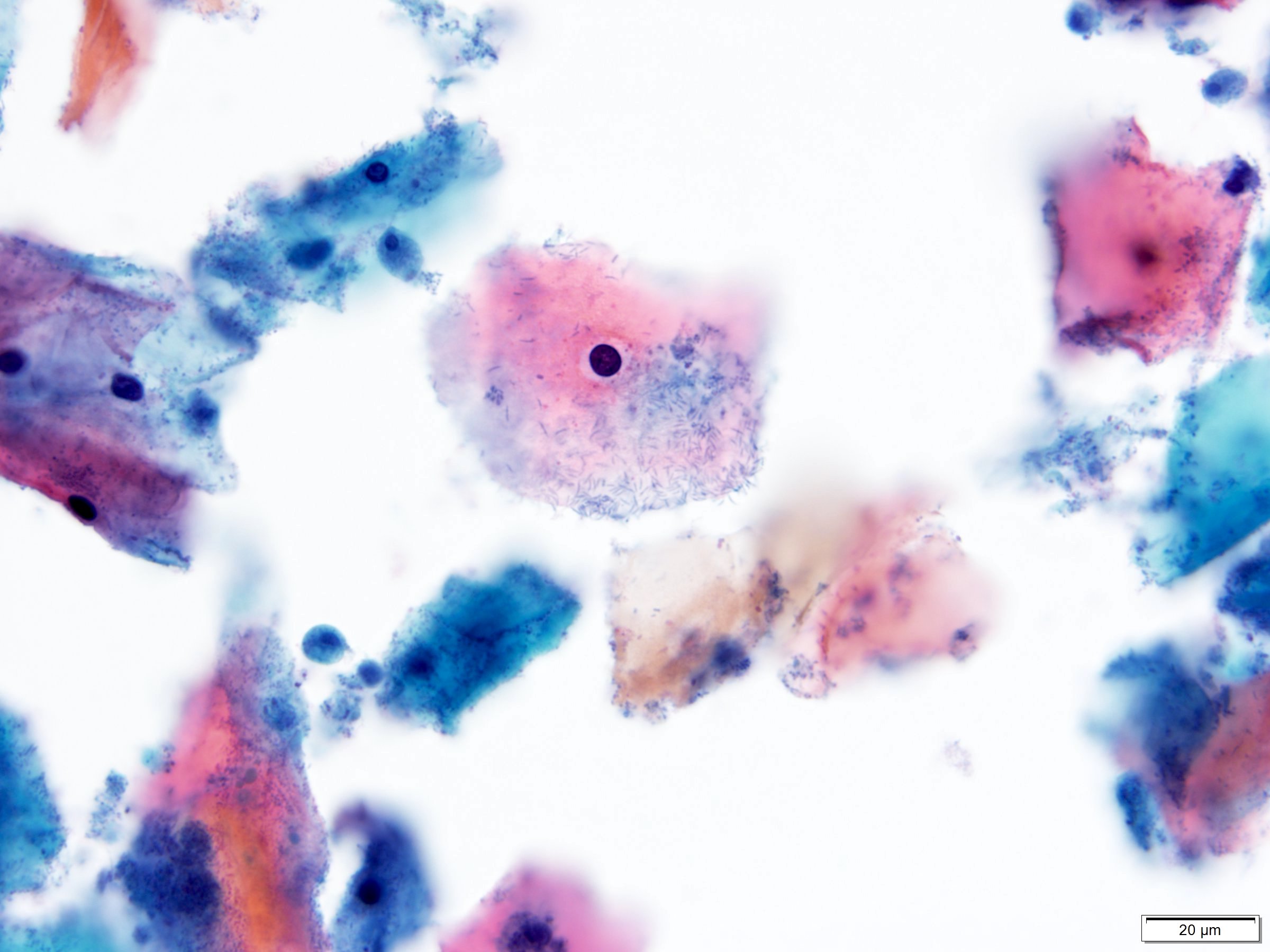
Lactobacillus
Aka Bacillus vaginalis
Etio NF seen on pap smears
luteal phase cannot survive in alkaline media
menstrual flow increases pH
cytology blue thick rods seen on top of intermediate squames
lyse glycogen rich intermediate cells
cytolysis bare nl sized IMC nuclei
abundant bacterial rods
Media pathoutlines
Shift in Flora
Micro short bacilli/coccobacilli, no lactobacilli
filmy appearance, clue cells
note mc gardnerella, not always
Glycogenated squames
{kind=link}
{kind=link}
Parakeratosis
{kind=link}
Hyperkeratosis (leukoplakia)
Follicular cervicitis
Bethesda system
Media Bethesda pathoutlines
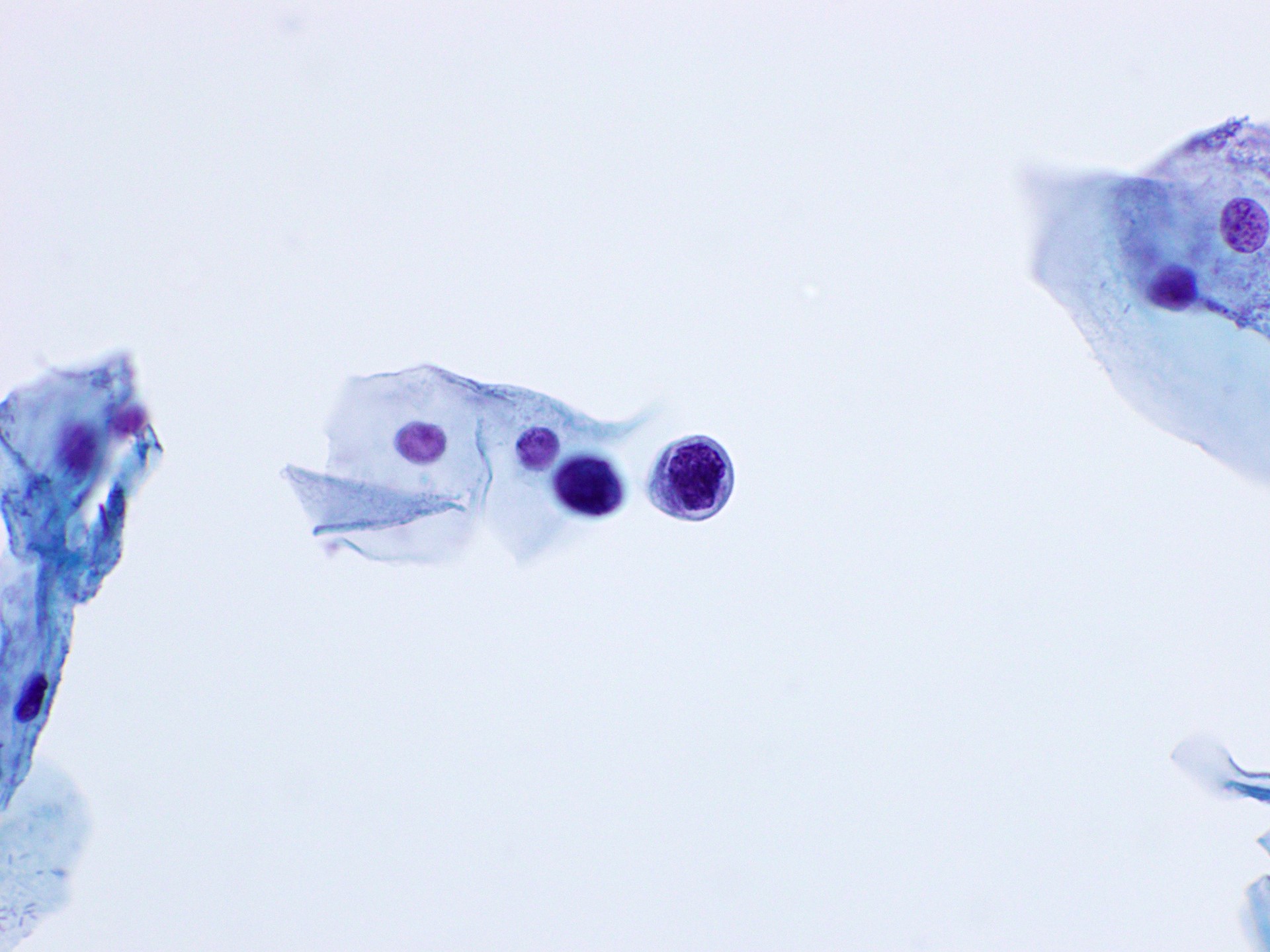
ASC-US
Cytology Nuclei size 2.5-3 x an intermediate squamous cell s
N:C slightly increased
Hyperchromasia minimal
Contour irregularities minimal
Cytoplasm Incomplete koilocytosis
CP cells appear larger and flatter (artifact)
LBP cells appear smaller with higher N:C
Rounding up of cells
Lack of flattening on the slide
clin repeat cytology in 6-12mo or HPV testing
Media pathoutlines
Atlas[55] pap[56] pap[57] pap[58]
{kind=link}
{kind=link}
{kind=link}
ASC-H
cytology cells occurring singly or in groups < 10 cells
cells are the size of metaplastic cells
nuclei nuclear size 1.5 to 2.5 x larger than normal
N:C may approximate HSIL
HPV-related changes are often not present
cytoplasm scant
ASC-H Patterns: Small cells with High N:C Ratios
aka atypical immature metaplasia
cytology cells occurring singly or in small groups < 10 cells
size of metaplastic cells
nuclei 1.5-2 x enlargement
N:C may approximate HSIL
ASC-H: Crowded sheet pattern
Cytology Typical atypical features
loss of polarity, dense cytoplasm
polygonal cell shape
fragments with sharp edge
CP cells may stream in strands of mucus
note needs immediate colposcopy
Media pathoutlines
{kind=link}
{kind=link}
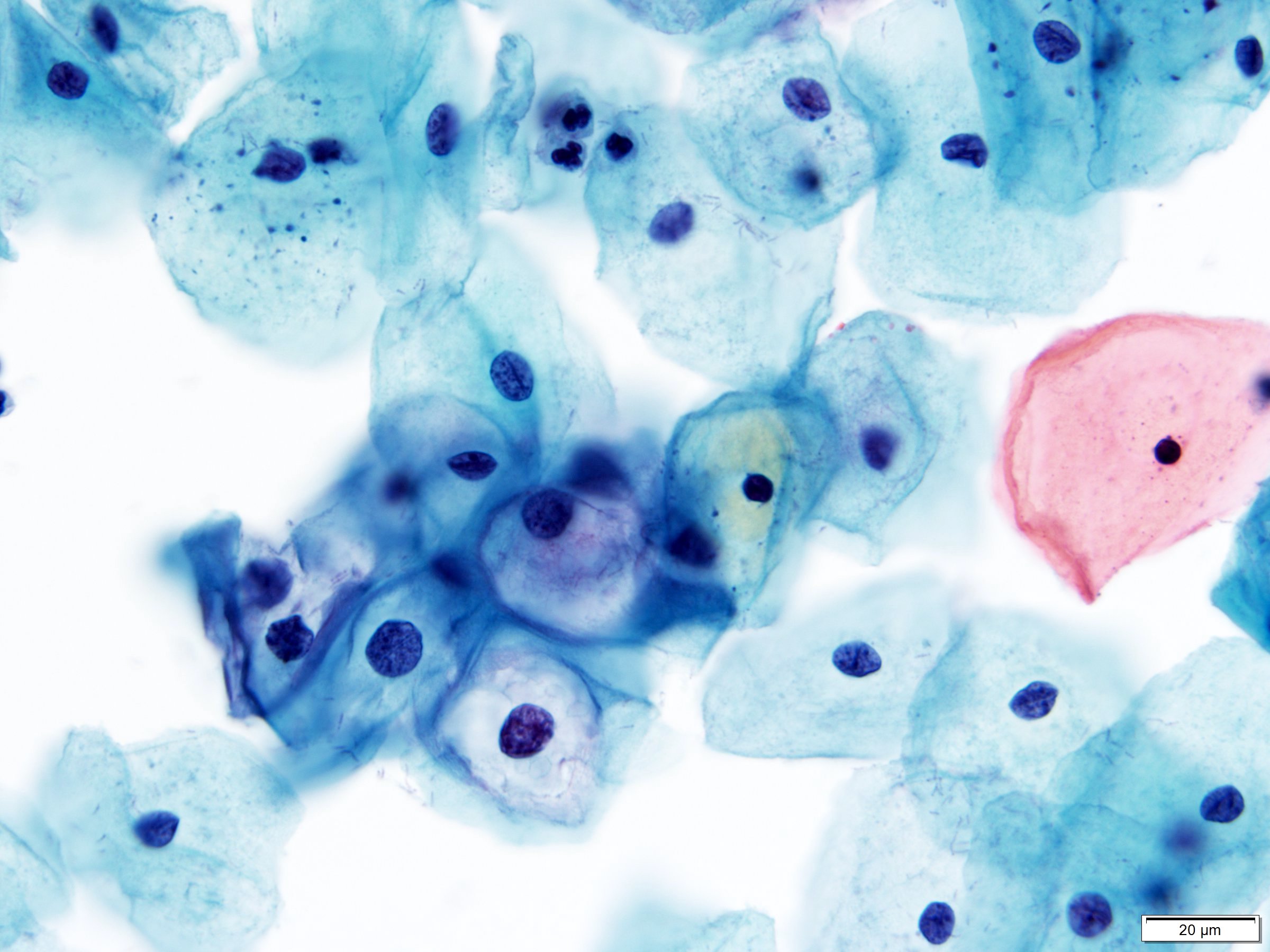
LSIL
cytology cells occur singly, inclusters, and sheets
nuclei enlarged ≥ 3 x an intermediate cell s
normochromatic to hyperchromatic
binucleation or multinucleation common
mebrane contours can be smooth or irregular
chromatin evenly distributed
granular, smudgy, or opaque
koilocytosis perinuclear cavitation
sharply delineated
N:C low but slightly increased
LBP appears similar to CP
Nuclei may show less hyperchromasia
clin repeat cytology in 6-12mo or HPV testing
colposcopy if persistent
note koilocytosis without nuclear abnormalities is not LSIL
Media pathoutlines
WSI WSI WSI WSI WSI WSI WSI WSI
LSIL Atlas[62] pap[63] pap[64] pap[65] pap[66]
{kind=link}
{kind=link}
{kind=link}
{kind=link}
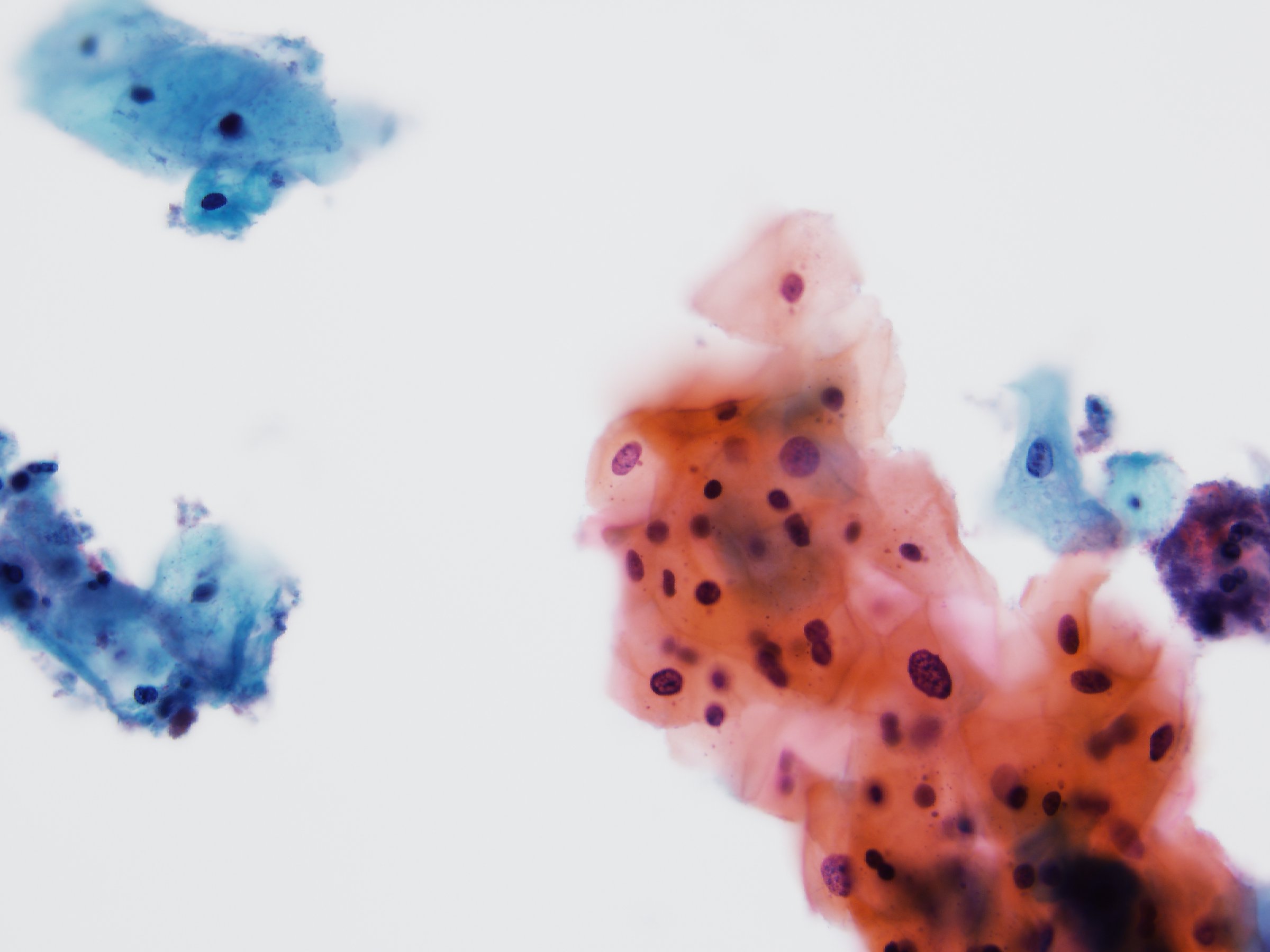
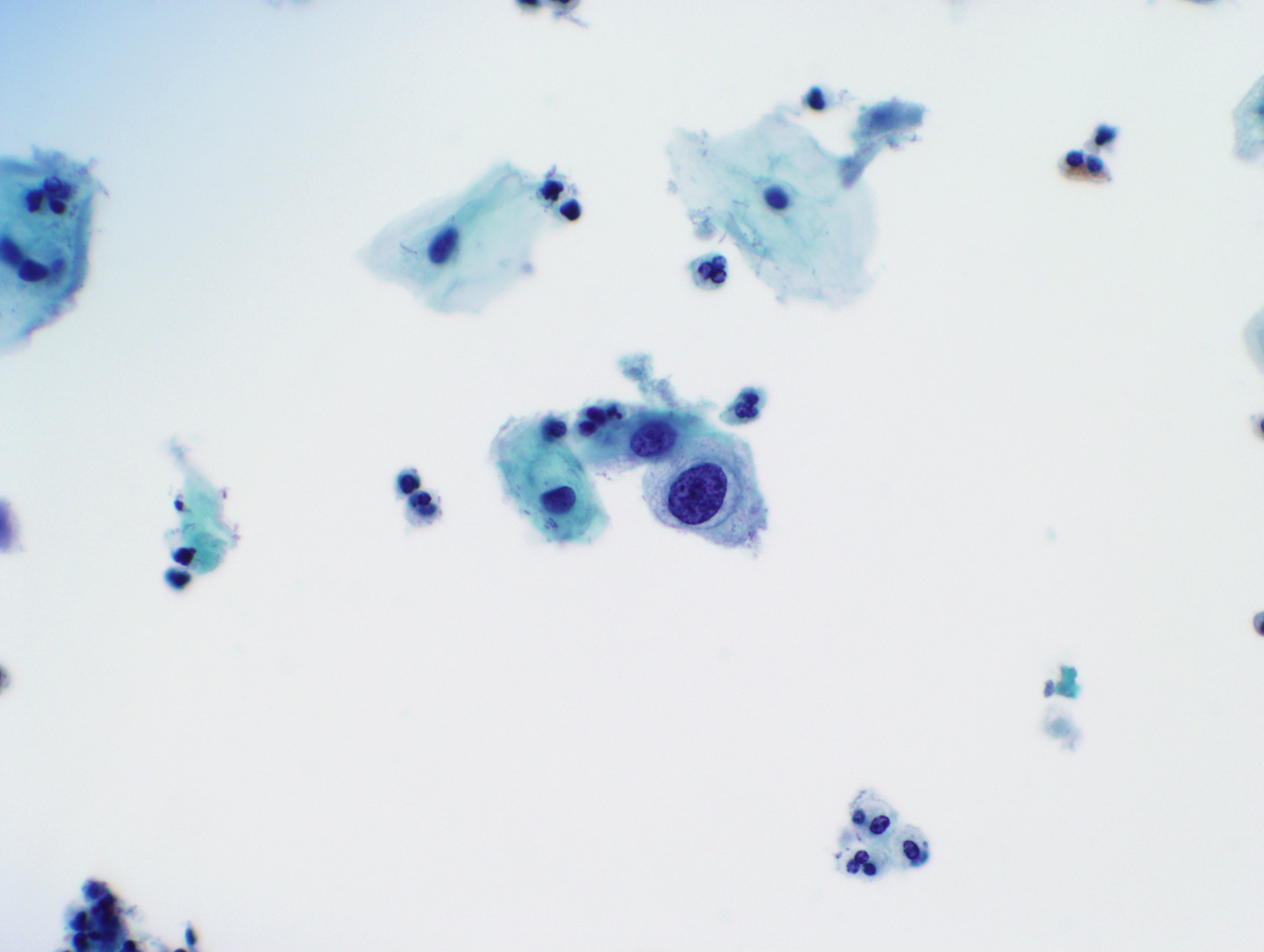
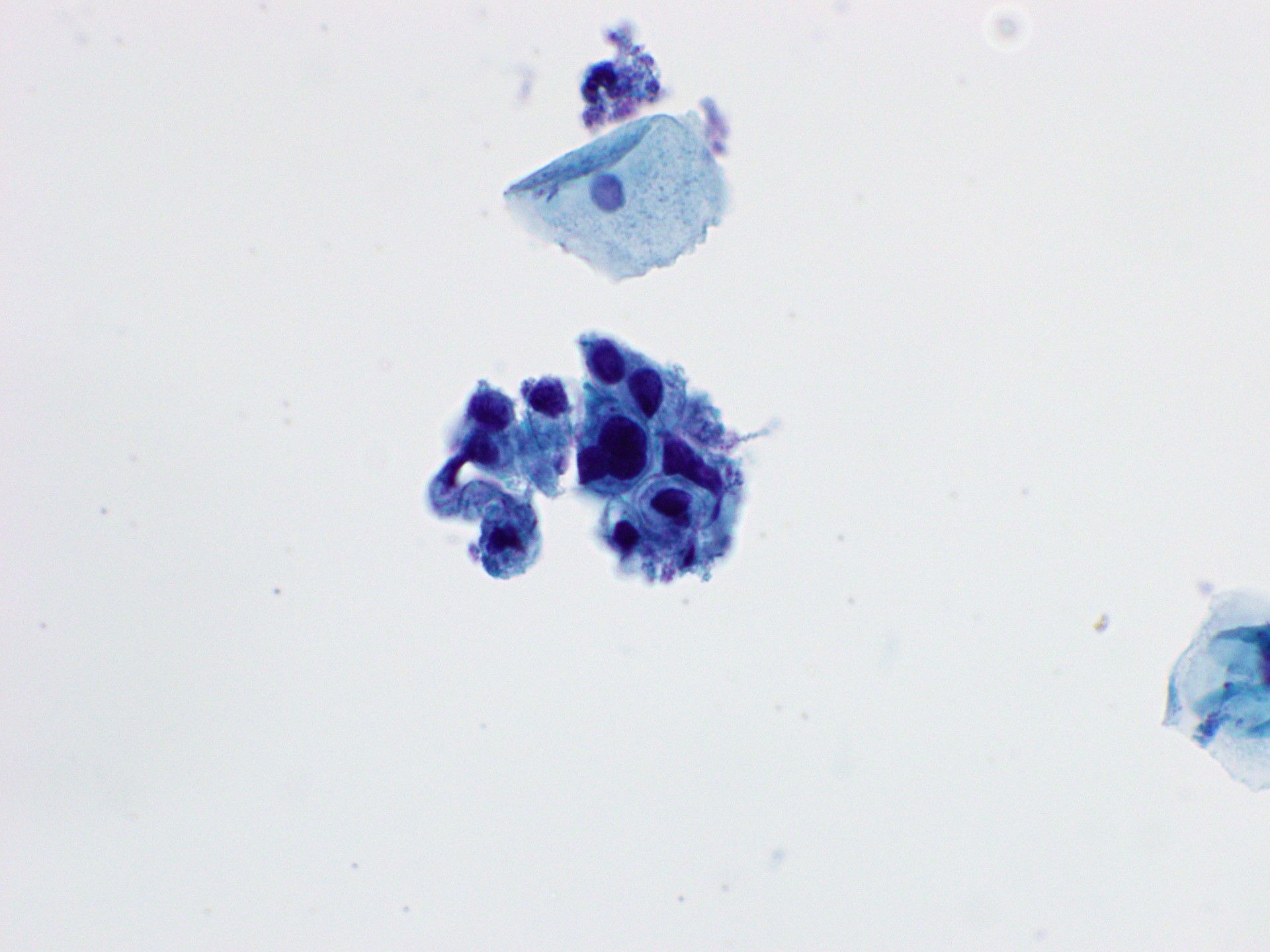
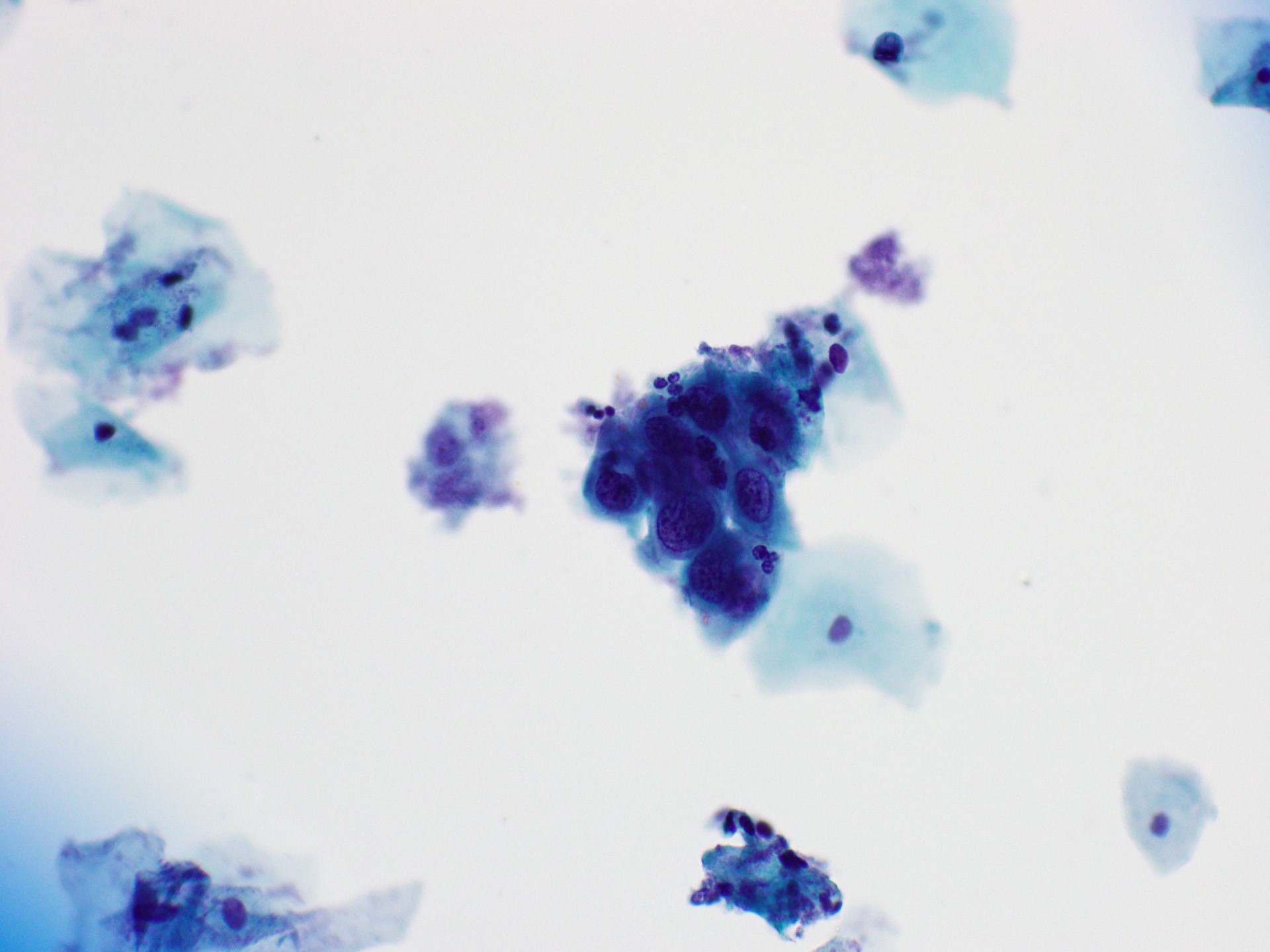
HSIL
cytology cells occur singly, in sheets, or syncytial aggregates
hyperchromatic groups seen in syncytial aggregates
cells are small than LSIL cells
nuclei enlargement varies, but N:C is always high
prominent indentations/grooves
usually hyperchromatic
normochromasia and hypochromasia may occur
chromatin evenly distributed
fine or coarse
nucleoli generally absent
cytoplasm can be immature, mature (keratinizing), or metaplastic
LBP more often see dispersed single cells
Less hyperchromasia
clinical needs immediate colposcopy or biopsy
note metaplastic type located in TZ or EC
most common type
small cell type reserve cells
located in TZ or EC
keratinizing dysplasia located on portio of cervix
Media pathoutlines
WSI collection (mod)
WSI collection (severe)
WSI WSI WSI WSI WSI WSI WSI WSI WSI WSI WSI
WSI WSI WSI WSI WSI WSI WSI WSI
pap[67] pap[68] pap[69] pap[70] pap[71]
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Glandular Lesions
Atypical glandular cells
Media pathoutlines
{kind=link}
Atypical of Endocervical Cells NOS
Tissue sheets & strips, pseudostratified, school of fish
More rounded and 3D on LBP w piled-up layers
Cytoplasm abundant but w increased NC
Nucleus hyperchromatic, enlarged but varied size/shape
Nucleoli occasional
Chromatin mildly irregular
Media webpage
Atypical of Endometrial Cells NOS
Clin Postmenopausal bleeding
HRT
Tissue 5-10 cell 3D groups, poorly defined cell borders
Nuclei enlarged, crowded
Hyperchromatic (esp on LBP)
Cytoplasm scant, often vacuolated
Nucleoli small (more prominent on LBP)
Media WSI
Carcinoma
media WSI collection[74]
Squamous cell carcinoma
Non-keratinizing (including basaloid)
Cytology cells syncytial aggregates & single cells
cell size somewhat smaller than HSIL
Nuclei irregular contours
coarse chromatin with clearing
nucleoli may be prominent
cytoplasm indistinct cell borders, high N:C
background tumor diathesis, necrotic debris
broken down blood elements
LBP lower tumor cellularity
Cells rounded up ─ may appear glandular
Clinging diathesis
Keratinizing
Cytology cells mostly single cells, aggregates less common
Marked variation in cell size & shape, eg tadpole cells
Nuclei vary markedly
Irregular nuclear membranes
Dense opaque nuclei often present
Coarse chromatin with clearing
Macronucleoli less common[75]
Cytoplasm frequently orangeopilic and keratinized
Background tumor diathesis less common[76]
Cytoplasm Heavily keratinized, NC low to hig, keratin pearls
tadpole cells, spindle cellls
Nucleus hyperchromatic
Chromatin dense or coarse
Nucleoli uncommon, also tumor diathesis uncommon
Adenocarcinoma
Endocervical Adenocarcinoma in situ (AIS)
Tissue strips, rosettes, feathering, stratified, crowding
Cytoplasm scant, finely vacuolated, unclear borders
Nucleus NC 2:1[77], oval-long
memb smooth-irregular, notching, thickened
Chromatin coarse, evenly distributed, hyperchromatic
Nucleoli variably present
Media webpage
Endocervical Adenocarcinoma
Cytology cells occur singly, 2D/3D clusters, or syncytial aggregates
Nuclei enlarged, pleomorphic, membrane irregularities
irregularly distributed chromatin with clearing
macronucleoli
cytoplasm finely vacuolated
background tumor diathesis common
LBP cell groups are denser and more spherical
more frequently isolated tumor cells
chromatin more vesicular
tumor diathesis clinging to the surface of groups
Endometrial Adenocarcinoma
Cytology cells occur singly or in small tight clusters
loss of polarity
Nuclei enlargement may be mild but larger in high-grade
Hyperchromasia moderate
Irregularly distributed chromatin with clearing
cytoplasm scant, cyanophilic, often vacuolated
bag of polys ─ intracytoplasmic neutrophils
background tumor diathesis may be present, best on CP
finely granular or watery
Media WSI WSI WSI WSI WSI WSI WSI WSI WSI WSI
─ Cyto ─ Thyroid
Media FNA-general pathoutlines
molecular testing in FNA pathoutlines
ultrasound pathoutlines
Bethesda system diagnostic categories pathoutlines
adequacy pathoutlines
unsatisfactory pathoutlines
Inadequate
Criteria Cellularity < 6 groups of 10 follicular cells
Cyst fluid only
Media pathoutlines
Unsatisfactory
< 6 groups of well preserved, well stained follicular cell groups with 10 cells each
Poorly prepared, poorly stained or significantly obscured follicular cells
Cyst fluid, with or without histiocytes and < 6 groups of 10 benign follicular cells
Media pathoutlines
Benign
Criteria consists of colloid and benign follicular cells
Watery colloid
Thick colloid
Note usually nodular hyperplasia on resection
Benign
Media pathoutlines
Follicular nodular disease
AKA colloid nodule, hyperplastic nodule
adenomatous nodule, benign follicular nodule
Cytology Colloid Watery Forms folds or lacunae
Thick Has a hyaline quality
stained-glass cracking appearance
Cells monolayered, honeycomb-like
occasionally 3D but retain polarity
minimal crowding or overlapping
Nuclei monomorphic, round to oval
Slight anisonucleosis allowed
Chromatin finely granular
Nucleolus inconspicuous or absent
Cytoplasm Delicate, poorly defined cell borders
Oncocytes granular cytoplasm
Central round nucleus
Prominent nucleolus
May show large cell dysplasia
+/- hemosiderin or lipofuscin pigment
papillary hyperplasia fv cores are rare
remain in flat sheets
no PTC nuclei
MΦ, often containing hemosiderin
Reparative changes, esp if cystic[78]
Cystic degeneration, reparative stretched cells
Note includes colloid nodule
hyperplastic nodule, adenomatous nodule, or benign follicular
nodule
Graves disease
Cytology Cells flat sheets, loosely cohesive groups
Typically not hypercellular
Cytoplasm abundnat, foamy, delicate
Nuclei enlarged & vesicular
Nucleoli prominent
Flame cells cytoplasmic vacuoles w pink frayed edges
Lymphocytes usually not prominent
If present, grooves and chromatin clearing non diffuse
Note treated GD prominent microfollicular architecture
nuclear overlapping and crowding
considerable anisonucleosis
Thyroiditis
Lymphocytic Thyroiditis
Cytology Cells Polymorphic lymphoid cells
Benign follicular cells
Oncocytic cells
Nucleoli Prominent in oncocytic cells
Cytoplasm Granular in oncocytic cells
scant to moderate in lymphoid cells
Granulomatous Thyroiditis
Cytology cells granulomas with multinucleated giant cells
Early many neutrophils and eos (~acute thyroiditis)
Later hypocellular
Giant cells eating colloid
Scant degenerated follicular cells
Involutional stage
Absent inflm cells and giant cells
Often insufficient for eval
Media WSI
Acute Suppurative Thyroiditis
Cytology cells few reactive follicular cells
Mostly neutrophils
Other aw necrosis, fibrin, MΦ, blood
Occasionally background bacteria or fungi
Riedel Thyroiditis
Epid rarest form of thyroiditis
Etio manifestation of IgG4-RD
Clin firm & fixed thyroid
fibrosing in other organs
cytology cells often acellular
rare inflm cells
other collagen strangs
bland spindle cellls
absent colloid & folllicular cells
Thyroglossal duct cyst
Site anterior midline, below hyoid, above thyroid isthmus
Cytology predominantly proteinaceous material & inflm cells
degenerated squamous or ciliated columnar cells
Bronchial cleft cyst
Cytology Mature squamous cells and anucleated squames
Atypia of undetermined significance
Criteria atypia insufficient for FN/OFN or SF categories
Media pathoutlines
Follicular neoplasm
Cytology Cells highly cellular, uniform follicular cellls
Microfollicle mc arrangement
flat or 3D groups
circumference < 15 cells
in circle > 2/3 complete
crowding & overlapping
Crowded groups, trabeculae
single cells infrequent
Nuclei normal size, round
Chromatin clumpy, mild hyperchromasia
Nucleoli absent or inconspicuous
Cytoplasm scant or moderate
Absent oncocytic changes
INPI, true papillae
Multinucleated cells
Potential NIFTP/FVPTC Nuclei larger
irregular contours/grooves
Chromatin clearing
Lack true papillae
Absent or very rare INPI
DDx Parathyroid GATA3, PTH, chromo, synapto, CD56+
TTF1, Tgb, calcitonin-
PTH in needle washout of FNA useful
Note cystic degeneration uncommon
Media pathoutlines
Follicular neoplasm ─ oncocytic
Cytology Cells almost exlcusively (> 75%) oncocytes
isolated cells, sheets, or crowded groups
Cytoplasm finely granular
Blue or gray-pink on Wright
Green on Pap, pink on H&E
Nucleus enlarged, eccentric, round
Binucleation common
Nucleolus prominent
Atypia small cell high N:C
Large cells 2x anisonucleosis
Sometimes Transgressing vessels
Intracytoplasmic colloid inclusions (lumens)
Absent high-grade features (necrosis, increased mitoses)
PTC nuclei (as in oncocytic PTC)
Colloid and macrofollicles
Abundant lymphs & plasma cells (excluding blood)
Mol PPARG rearrangements and BRAF V600E absent
Media pathoutlines
Suspicious for malignancy
Media pathoutlines
Malignant
Media pathoutlines
Salivary neoplasms
Mucoepidermoid carcinoma
Micro cellularity depends on grade
low-grade produces abundant background mucin and macrophages due to cystic change, often with few epithelial tissue fragments
Mucinous cells have goblet cell type single large vacuoles or foamy oval regions of mucin (pink by Pap, magenta by Giemsa) and are scattered among polygonal intermediate cells in tissue fragments, as well as cohesive sheets of squamous (epidermoid) cells with denser cytoplasm and well-defined borders but lacking keratinization
High-grade carcinomas are readily identifiable as malignant due to their atypical epidermoid cells with a lesser number of interspersed goblet-type mucinous cells, more prominent nuclear pleomorphism, larger nucleoli, necrosis, and (in some cases) mitoses
Adenoid cystic carcinoma
Variably cellular
Sheets with microcysts or cribriform, tubular, or complex tissue fragments and a lesser number of single cells
Monotonous population of basaloid cells with a high N:C ratio and bland, oval to angulated nuclei with evenly dispersed dark chromatin and indistinct nucleoli
The tumour matrix is usually sharply defined, balled up or branching, thick, and pale eosinophilic to virtually non-staining (Pap) and magenta (Giemsa); in some cases it forms a rim surrounding basaloid tumour cells
Epithelial-myoepithelial carcinoma
Usually highly cellular
Two cell types, with tightly cohesive tubules or balls of basaloid epithelial cells with a high N:C ratio surrounded by larger myoepithelial cells with clear cytoplasm and oval nuclei
Loosely cohesive tissue fragments of myoepithelial cells and stripped oval nuclei in the background
Variable (but usually small) amount of eosinophilic (Pap) and magenta (Giemsa) matrix including stromal balls
Papillary Carcinoma
Cytology Cells arranged in papillae, monolayer sheets, 3D groups
Cellular swirls ( onion-skin or cartwheel )
Nuclei enlarged & crowded nuclei, often molded
Longitudinal nuclear groove
Intranuclear pseudoinclusions (INPI)
Thick nuclear membranes
Chromatin Powdery
Nucleoli macronuceoli or micronucleoli
Central or marginally placed
Other Psammoma bodies
Multinucleated giant cells
Colloid variable, may be bubble-gum like
Oncocytic or squamous metaplasia
Hobnail features, eg around psammoma bodies
Hemosiderin-lade MΦ representing cystic Δ
Variable lymphocytes, eg in underlying thyroiditis
Absent Necrotic debris is extremely rare for PTC
Mol MAPK, BRAF V600E, RAS[79]
NIFTP
Cytology ≥ some degree of atypia present (unlike benign nodule)
Lack true papillae and psammoma bodies (unlike PTC)
Encapsulated Follicular Variant PTC and NIFTP
Cytology PTC features subtle, partial, and focally displayed
Cells low to moderate cellularity
Follicular architectural pattern
Nuclei enlargement, elongation, chromatin clearing
Thick nuclear membranes
Absent IPNIs and nuclear grooves (may be rare)
True papillae, PBs, sheet-predominant pattern
Mol RAS, or RAS-like (PPARG & THADA) (like follicular neoplasms)
RET & RET-like (BRAF V600E) absent (unlike PTC)
Follicular Variant PTC with Infiltrative Growth
Mol BRAF V600E ( BRAF -like PTCs )
Prog frequent LN mets, risk recurrence
Media WSI follicular variant
Macrofollicular Variant PTC
Epid very rare
Cytology cells monolayered sheets or variably sized follicles
Nuclei subtle and patchy PTC nuclei
Absent PBs and papillary structures
Cystic Variant PTC
Cytology cells typically small groups w irregular borders
histiocytoid (hypervacuolated)
Nuclei definitely PTC-like, but less fine chromatin
Other hemosiderin-laden MΦ
Media WSI WSI cystic variant
Oncocytic PTC
Cytology Cells predominantly oncocytic cells
Nuclei definitely PTC-like
Absent lymphocytes (or few in number)
Media WSI oncocytic variant
Warthin-Like Variant PTC
Cytology nuclei convincingly PTC nuclei
other lymphoplasmacytic background
Lymphs permaeated fibrovascular stalks
Tall Cell Variant PTC
Epid elderly patients, M > F
Criteria >30 % tall cells
Cytology nuclei PTC changes present
larger and longer
Chromatin more granular
Nucleoli prominent and central
Other fewer PBs
more INPIs (often multiple wi a nucleus)
mol BRAF V600E in vast majority
TERT promoter mutations also common
prog mc aggressive variant, bad even if only 10% tall cells
frequent extrathyroidal extension and vascular invasion
higher incidence of recurrence, neck involvement, mets
Columnar Cell Variant PTC
Epid rare variant
Cytology cells arranged in papillae, flat sheets, or clusters
pseudostratified columnar
cytoplasm supranuclear & subnuclear vacuoles
nuclei PTC changes present, but are less prominent
generally few INPI or nuclear grooves
chromatin more hyperchromatic
other ~secretory endometrium or tubular adenoma
generally lack colloid or cystic changes
ICC PAX8+, most also CDX2+
Mol BRAF V600E, TERT promoter
prog aggressive in older patients
Solid / Trabecular PTC
Epid rare variant
Criteria > 50% solid, trabecular, nested, or insular
< 50% follicles,papillae, colloid
Cytology cells syncytial 3D fragments, microfollicles, trabeculae
nuclei PTC features
absent true papillae with fibrovascular cores
mol RET, NTRK, TERT promoter
Diffuse Sclerosing PTC
Epid more common in kids and young adults
esp w hx nuclear fallout
Cytology cells mod-high cellularity
3D ball-like clusters, intermingling inflm cells
Cytoplasm dense w distinct cell borders
Unilocular cytoplasmic vacuoles common
Nuclei PTC changes present
Chromatin less pale
Fewer IPNIs and nuclear grooves
Other squamous metaplastic changes
background Numerous lymphs and PB
Absent colloid (or only scant)
Mol NCOA::RET in the setting of radiation/fallout
Prog vs. Conventional disease free survival but ~mortality
note diffuse inolvement, extensive LVI, prominent fibrosis
Hobnail Variant PTC
Epid rare variant
Cytology cells loss of polarity & cohesiveness
Nuclei eccentric
Soap bubble-like INPIs
Typical PTC features present
Cytoplasm tapered, comet- or teat drop-like
Mol BRAF V600E in vast majority
Prog aggresive PTC subtype
Medullary Carcinoma
Cytology cells moderate to high cellularity
Non-cohesive cells and syncytial aggregates
Nuclei round to elongated, eccentric
Coarsely granular chromatin ( salt and pepper )
Binucleation common
INPIs uncommon
Nucleoli mostly inconspicuous
Cytoplasm granular, quantity variable
May have vacuoles, melanin, and lumina
Other dense amyloid resembling thick colloid
Absent nuclear grooves
ICC calcitonin+, CEA+, TTF1+, synapto+, chromo+
PAX8-, Tgb-
Cellular, discohesive, plasmacytoid
polygonal to spindled
Salt and pepper chromatin
Mol RET, eg MEN2A and MEN2B
Anaplastic Carcinoma
Epid > 50 yo, female
Clin hard, nodular, rapidly growing mass
Symptoms from neck compression
Lymphadenopathy and distant mets, mc lungs
History of long-standing goiter and euthyroid
Cytology cells variable cellularity, usually at least moderate
Eouthelioid and/or spindle-shaped
Small to giant, can be plasmacytoid or rhabdoid
Nuclei enlarged, irregular, extreme pleomorphism
Chromatin clumped with parachromatin clearing
Nucleoli prominent and irregular
Other abscess-like neutrophil predominant inflm
ICC PAX8 & keratin+ (can be focal)
TTF1-, Tgb-
Mol TP53, CTNBB1, RAS, BRAF V600E, TERT promoter
Papillary Hyperplastic Nodule
Clin < 3 cm, solitary, teenage F, +/-hyperfunctioning
Cytology partly cystic, darker nuclei than PTC
Media video segment
Lymphoma
Cytology Cells marked cellularity, non-cohesive
background lymphglandular bodies
Absent oncocytes, follicular epithelial cells, plasma cells
MZL cells 2x mature lymphocyte
nuclei vesicular chromatin, small nucleoli
DLBCL nuclei coarse chromatin, prominent nucleoli
Cytoplasm abundant, basophilic
Bethesda
I Unsat Repeat FNA
II Benign < 5 % Clin fu
III AUS/FLUS < 10-30 % Repeat vs Mol
IV Follicular Neo < 25-40 % Lobectomy
V Suspicious < 60-75 % Thyroidectomy
VI Malignant 100% Thyroidectomy
Media Benign video
Atypia video
Follicular video
Other Tumors
Cribriform morular thyroid carcinoma
Cytology Cells papillary-like formations
Background spindle cells
Background histiocytes
Nuclei hyperchromatic, pseudostratified
INPIs, nuclear grooces, few other PTC features
Other eddy formation (morules)
Absent colloid, PBs, multinucleate giant cells
ICC TTF1+, nuclear β-catenin+
Tgb-, PAX8- or weak
Mol Wnt/β-catenin
Hyalinizing trabecular tumor
Epid rare thyroid tumor, vast majority women
Cytology cells round or spindle shaped
Radiating from hyaline core
Nuclei numerous INPIs & nuclear grooves
Cytoplasm abundant, eosinophilic or amphophilic
Other occasional PBs
Cytoplasmic paranuclear yellow bodies
Absent papillary, sheet-like fragments
ICC TTF-1+, Tgb+, membranous MIB1/Ki-67
Calcitonin-
Mol GLIS rearranged
High-Grade Follicular Cell-Derived Non-Anaplastic Thyroid Carcinoma
Aka poorly diff thyroid carcinoma
─ Cyto ─ Serous fluids
Types of cells
Benign Mesothelial cells
Cytology Cells flat sheets, usually do not cluster in 3D
Microvilli form intercellular space ─ window
Cytoplasmic arms hugging adjacent cells
Nuclei round with vesicular chromatin
Low N:C, smooth contour
Nucleoli prominent or inconspicuous
Cytoplasm abundant, dense
Two-tone, denze perinuclear zone
Reactive mesothelial cells
Cytology nuclei marked atypia, enlargement, variation
Prominent nucleoli
N:C in the normal range
Binucleation and multinucleation common
Can be knobbly, forming daisy cells
May form 3D clusters containing < 50 cells
May show signet-rings mesothelial nuclear features
non-foamy vacuoles
Note seen in cancer patients on rtx/ctx, esp for lung/breast
Histiocytes
Cytology granular or vacuolated cytoplasm
Agggregates or isolated cells
IHC CD68, CD163
Types of Effusions
Transudative Effusions
Etio imbalance in hydostatic and oncotic pressure
Clin CHF, cirrhosis, nephrotic syndrome, atelectasis
Hypoalbuminemia, peritoneal dialysis
Criteria < 0.5 PF:serum protein ratio
< 0.6 PF:serum LDH ratio
PF LDH < 2/3 ULN in serum
Note low specific gravity, low fluid protein, low LDH
Exudative Effusions
Etio injury to mesothelium, eg by inflm or malignancy
Clin connective tissue disease, pneumonia
Pancreatitis, sarcoidosis, chylothorax
Malignancy
Criteria > 0.5 PF:serum protein ratio
> 0.6 PF:serum LDH ratio
PF LDH > 2/3 ULN in serum
Note high specific gravity, high fluid protein, high LDH
Lymphocytic Effusions
Etio chronic inflammation, TB, chylous effusion
Lymphoma or non-lymphoid malignancy
DDx LPD monomorphic small lymphocytes
Atypica lymphoid cells
Note a few lymphocytes in a chronic effusion is common
Reactive if mostly CD3+ T cells w scattered CD20+ B cells
Neutrophilic effusions
Etio bacterial pneumonia, TB, chest surgery, lung abscess
Criteria exudative with predominance of neutrophils
Fluid grossly purulent
Note may occur in the context of malignancy
Eosinophilic Effusions
Etio idiopathic mc
Pneumothorax, hypersensitivity reaction
Parasitic infection, prior procedure
Criteria abundant eosinophils ( > 10 % cellularity)
Note rarely associated with malignancy
Chylous effusion
Etio fatty leakage from thoracic duct
Often caused by lymphoma
Criteria rich in triglycerides and chylomicrons
Mostly lymphocytes
Lipophages and mesothelial cells
Tuberculous effusions
Cytology abundant T lymphocytes, absent mesothelial cells
Clumps of exudated fibrin and trapped cells
Rheumatoid effusion
Aka Rheumatoid pleuritis
Cytology multinucleated giant cells
elongated histiocytes
Granular and necrotic debris
DDx low grade lymphoma
Systemic Lupus Erythematous
Aka SLE
Cytology LE cells neutrophil or macrophage
Contains hematoxylin body[80]
Benign entities
Collagen balls
Epid seen in women only
Site pelvic washings and peritoneal washing specimens
Clin non-specific finding
Cytology fragments of collagen mixed w mesothelial cells
Smooth contours
Endometriosis
Cytology endometrial epithelial and stromal cells in sheets
Hemosiderin-laden histiocytes
Endosalpingiosis
Cytology cuboidal-columnar ciliated epithelial cells
Smooth nuclear membrane, fine chromatin
small clusters or branching tubular structures
International System
Media pathoutlines
Non-Diagnostic
Criteria volume < 50ml not be sufficient to exclude malignancy
cellularity degree for inadequate not defined
Quality poor cell preservation, artifact
Hemorrhage, contaminants
Note report should explain why it is inadequate
Negative for malignancy
Criteria Benign cellular and noncellular findings
prog 21% risk of malignancy
Note constitutes majority of samples
Atypia of unknown significance
Criteria insufficient criteria for malignancy
Prog 66% risk of malignancy
Note category should be avoided
May be used while awaiting ancillary studies
Suspicious for malignancy
Criteria features suspicious but not definitive
Clin established malignancy in most pt
Prog 82% risk of malignancy
Note presence of second population (non mesothelial)
Malignant
Adenocarcinoma
Cytology 3D clusters, smooth borders, lack intercellualr windows
nuclear enlargement, coarse chromatin
prominent nucleoli, nuclear overlap and irregularity
numerous cytoplasmic vacuoles
lacunae around tumor cell clusters (cell block)
colorectal dirty necrosis
overt cytoplasmic vacuolization
ductal breast cannonball 3D clusters
pearl form or cell-in-cell arrangement
Lobular breast intracytoplasmic lumina
dispersed individual plasmacytoid cells
Magenta bodies ─ intracytoplasmic vacuoles
Cells smaller than other adenocas
Lack marked atypia or pleomorphism
gastric signet-ring foamy vacuoles
poor vacuolar borders
pancreas marked anisonucleosis
chromatin coarse, nucleoli prominent
cytoplasm granular to vacuolated
lung community border (smooth border)
nuclei hyperchromatic, eccentric
cytoplasm scant to abundnat, vacuolated
media WSI gastric signet ring cell adenoca
WSI lobular carcinoma (breast primary)
Papillary thyroid carcinoma
Cytology abundant papillae
Nuclei enlarged, overlpping, intranuclear grooves
Pseudoinclusions
IHC (+) TTF1, napsin A, Tgb, PAX8
Epithelial marker MOC31, CEA, BerEP4
Small cell carcinoma
cytology cells 3D hyperchromatic clusters
small chains, or isolated cells
nuclei nuclear molding, crowding
Chromatin salt-and-pepper
Nuceoli inconspicuous
cytoplasm scant
paranuclear blue bodies
IHC (+) synaptophysin, CD56, INSM1
IHC (-) chromogranin
DDx poorly diff adenocarcinoma
lymphoma
Merkel cell carcinoma
note frequent mitoses, necrosis, apoptotic bodies
"blue strips" from crush artifact
small cell variant 2 3 times WBC size
large cell variant can be larger
media WSI small cell lung carcinoma
Squamous cell carcinoma
Cytology Cell clusters loosely formed
Syncytial sheets or singly scattered
Intercellular window absent
Nuclei large or pyknotic
Nucleoli may be prominent
Chromatin smudgy
Cytoplasm dense, elongated, often two-toned[81]
Intercellular bridges
IHC (+) CK5/6, p40, p63
IHC (-) napsin-A, TTF-1
DDx Poorly diff adenocarcinoma
Primary Effusion Lymphoma
Epid HIV patients
Etio HHV8, often co-infected with EBV
Cytology larger hyperchromatic round nuclei w nucleoli
Varying amounts of cytoplasm
Melanoma
Cytology Loose clusters, singly scattered large cells
Nuclei eccentrically located
Nuclear pseudoinclusions
Nucleoli large and prominent
Cytoplasmic melanin
Mirror image binucleation
IHC (+) SOX10, S100, HMB45, melanin A
Ovarian Serous Carcinoma
cytology cells papillary clusters w fibrovascular cores
nuclei large, round to ovoid
coarse chromatin, prominent macronucleoli
cytoplasm scant, vacuolization,
occasional psammoma bodies
IHC (+) PAX8, PAX2, WT1, p53 anl
DDx reactive mesothelial cells PAX8-, PAX2-, BerEP4-
Media WSI ovarian serous carcinoma
Metastatic Urothelial Carcinoma
cytology cells tumor clusters or sheets
squamoid appearance
nuclei pleomorphic, hyperchromatic
coarse granular chromatin
prominent small nucleoli
cytoplasm dense, distinct cell border
IHC (+) GATA3, PAX8
IHC (-) p40
DDx SCC p40+, GATA3-, PAX8-
Mesothelioma
Clin effusion described as honey like
Cytology Clusters of 20- 50 cells with scalloping borders
Intercellular window present
Nuclei hyperchromatic
Chromatin coarse
Nucleoli prominent
Cytoplasm vacuolated
psammoma bodies
IHC (+) PanCK, D2-40/podoplanin, calretinin
IHC (-) BAP1, MTAP
Mol CDKN2A deletion (p16)
Media WSI Mesothelioma
WSI WSIMesothelioma, epithelioid type
Lymphoma
Media WSI ALCL, ALK-positive
WSI mantle cell lymphoma
WSI PTLD, DLBCL type.
Leiomyosarcoma
cytology cells pleomorphic malignant spindle cells
loosely cohesive groups
nuclei cigar-shaped, hyperchromatic
irregular membranes
cytoplasm abundant, elongated
eosinophilic with fibrillary appearance
numerous mitotic figures
inflammatory cells and necrotic debris
IHC (+) SMA, desmin, myogenin
Note
Epithelioid Angiosarcoma
cytology cells isolated large epithelioid cells
occasional papillary groups
nuclei hyperchromatic, coarse chromatin
irregular nuclear membranes
prominent nucleoli
cytoplasm may be vacuolated
IHC (+) CD31 positive in nearly 100%, more specific than CD34, cytokeratin positive in ~50%
DDx metastatic carcinoma distinguishing feature here
epithelioid mesothelioma distinguishing feature here
note specimen often bloody, CD31 preferred marker for specificity
Other malignancies
Media WSI clear cell sarcoma
WSI WSIEpithelioid hemangioendothelioma
WSI Ewing Sarcoma
WSI glioblastoma
WSI Merkel cell carcinoma
WSI oncocytic carcinoma, thyroid primary
WSI ovarian clear cell carcinoma
WSI papillary thyroid carcinoma
WSI SMARCB1/INI1-deficient neoplasm
WSI thymic carcinoma
─ Cyto ─ Respiratory
Cells
Respiratory columnar cells
Cytology Cilia with terminal bar
Note uncommon in exfoliated material
May originate in nasal cavity / nasopharynx
Goblet cells
Cytology wider than ciliated cells
Basal nucleus with distended supranuclear cytoplasm
Mucinous vacuoles
Note less predominant than ciliated columnar cells
Goblet cell hyperplasia seen in asthma
Basal or reserve cells
IHC (+) p40 useful internal control
Macrophages
Note presence confirms origin from alveoli
Squamous cells
Note in LRT represent reactive and metaplastic change
Collection methods
Sputum
Clin used to diagnose LRT infections, diffuse ILD
Adequacy need sufficient volume for at least 2 smears
need abundant alveolar macrophages
Broncheoalveolar lavage
Adequacy > 10 alveolar MΦ per 2mm2 (~20 per 10HPF)
Bronchial brushing and bronchial washing
Adequacy large number of ciliated columnar epithelial cells
Goblet cells, macrophages
Atypical or malignant cells
FNA
Adequacy presence of cyto features to explain clinical findings
I ─ Insufficient / Inadequate / Non-diagnostic
Criteria preparation artifact precludes eval
Excess blood or mucus obscures cells
Normal in the setting of masss/lesions
Sputum samples needs alveolar macrophages
Clin no useful info
Note any degree of atypia precludes this category
High risk of malignancy ~40%
Media pathoutlines
II ─ Benign
Criteria normal in the absence of mass
Presence of cilia
Note Sample Adequacy Criteria
adequate material to evaluate / define a lesion
Inflammatoryxs acute inflammation
pneumonia, abscess
Granulomatous sarcoidosis vs infection
Pulmonary infarction
Nodular amyloidosis
Viral pneumonia
Neoplasm Pulmonary hamartoma
Sclerosing pneumocytoma
Granular cell tumor
Media pathoutlines
Granular cell tumor
Cytology densely granular cytoplasm
bland polygonal cells
Media WSI
Pulmonary alveolar proteinosis
Etio impaired surfactant clearance by alveolar MΦ
mtn in surfactant protein or GM-CSF receptor gene
cytology globules of amorphous or fibrillar PAS+ casts
in background and wi macrophages
media pathoutlines
Lipoid pneumonia
Etio exogenous aspirated lipids (mineral oil, vaping)
Endogenous lung tissue / membrane breakdown
Cytology lipid droplets highlighted wih oil red O or sudan black
Note Usually incidental post mortem finding
Media pathoutlines
Pulmonary Hamartoma
Cytology Fibrillary myxoid stroma with bland spindle cel
Possible fragments of hyaline cartilage or adipose
Sheets of bland bronchiolar epithelium
Bronchiolar epithelium
Intranuclear cytoplasmic pseudoinclusions
Mol HMGI alterations
Media pathoutlines
WSI Pulmonary adenofibroma
Sclerosing Pneumocytoma
Cytology bland pneumocytes and spindle cells
cells form sheets and papillae
pneumocytes may be enlarged and atypical
intranuclear pseudoinclusions
stromal spindle elements in cores of pneumocytes
Solitary tracheobronchial papilloma
Cytology squamous scattered squamous cells
some anucleate
keratinizing and non-keratinizing
background inflammatory
background keratinous debris
no cellular debris or tumor necrosis
koilocytic atypia, rarely dysplastic
glandular enlarged ciliated columnar cells
singly scattered
Bronchial cell hyperplasia
Aka creola body
Cytology tissue fragments of columnar cells
palisading of peripheral cells
cilia present, N:C normal
nuclei oval, relatively uniform, +/- nucleoli
Basal cell hyperplasia / Reserve cell hyperplasia
Cytology cohesive sheets, small uniform cells
scant cytoplasm, high N:C
nuclei round, even chromatin, no nucleoli
may show maDturation toward columnar cells
background clean
note Normally firmly adhered to basement membrane
Rarely seen in sputum
Instrumentation causes forceful detachment
Reactive bronchial epithelium, repair and regeneration
Cytology Papillary tissue fragments, 3D or cohesive sheets
Large polygonal cells with abundant cytoplasm
Cilia may be lost
Nuclei enlarged and oval, smooth nuclear membrane , macronucleolus
Type 2 pneumocyte hyperplasia
Cytology reactive cells
seen individually, sheets, or in rosette-like clusters
Some large nuclei with large nucleoli
Cytoplasm may be vacuolated
Squamous metaplasia
Cytology Sheets and single cells
Round to slightly irregular nuclei
Variable to high N:C ratio
Variable chromatin, occasional nucleoli
Dense eosinophilic cytoplasm with some keratinization
Note only considered as precursor if atypical
Cytopathic changes in viral infection
Cytology CMV large cells with large round to oval nuclei
single large intranuclear viral inclusion
chromatinic rimming, an owl-eye appearance
basal cytoplasmic inclusions
HSV inclusion filling the entire nucleus
frayed nuclear envelope
dark degenerative nuclear inclusion bodies
often multinucleated giant cells
Adeno smudge cells, mild cellular enlargement
smudged nonpunctate chromatin
aw detached ciliary tufts (ciliocytophthoria)
Chemotherapy- and radiotherapy-related changes
Cytology squamous and respiratory epithelium affected
Enlarged cells with vacuolated cytoplasm,
smudged chromatin, large nucleoli
Squamous metaplasia
Enlargement of type 2 pneumocytes
Note Chemotherapy appear wi a few weeks
resolve wi a month or two
Radiation acute changes appear wi 6 mo
chronic changes persist for years
Curschmann s Spirals
Etio inspisated mucous, often seen in asthmatics
Cytology spiral-shaped mucus plugs
Note can be stretched up to 2cm
III ─ Atypical
crtieria inflammatory or infective changes
changes in radiation therapy or chemotherapy
changes that cannot be distinguished from neoplasm
often scant cells with some cells showing atypia
background often suggestive of neoplasm
necrotic or keratinous debris, thick mucin, or apoptotic cells
IV ─ Suspicious for Malignancy
criteria some features suggestive, insufficient number / quality
"bridging" of "atypical" and positive for malignancy
Note Interobserver variability is high
V ─ Malignant
Def unequivocal cytopathological features of malignancy
Media pathoutlines
Adenocarcinoma
Cytology 3D aggregates spheres and papillae
Flat sheets manifest acini and glands
Cytoplasm granular, finely vacuolated
large vacuoles may indent nuclei
mucin present
Nuclei solitary, eccentrically situated
slightly irregular membranes
finely granular chromatin
well developed nucleoli
lepidic may show intranuclear pseudoinclusions
may show nuclear grooves
micropapillary lack fibrovascular core
mucinous milder pleomorphism
drunken honeycomb
abundnant mucin
Media WSI Primary mucinous
WSI with EGFR mutation
Squamous cell carcinoma ─ well diff
Cytology Cellularity high
Nuclei central, large, angular, clumped chromatin
Pyknotic in keratinized cells
Nucleoli prominent
Cytoplasm orange (pap) in single keratinized cells
blue (giemsa) in single keratinized cells
Background necrotic debris
Relatively cohesive tissue fragments w keratin pearls
Background dirty due to central necrosis/cavitation
granulomatous and acute inflammation
note not possible to distinguished from metastatic
Squamous cell carcinoma ─ mod to poorly diff
Cytology High cellularity
Background necrotic debris
Nucleoli prominent
More cohesive tissue fragments, often flat sheets or 3D
Elongate cells w dense cytoplasm wo keratinization
Basaloid predominantly cohesive sheets
Palisading nuclei at the margin
note not possible to distinguished from metastatic
Cytology Single cells and flat sheets
Well defined membranes
Keratinization present
Cytoplasm polygonal, oval, irregular shapes
Nuclei oval to rectangular contours
centrally localized
coarse to pyknotic
hyperchromatic chromatin
nucleoli high grade
ICC at least one SCC marker+ and TTF1-
DDx NUT carcinoma[82]
Adenoid cystic carcinoma[83]
Neuroendocrine tumor
Epid 50s, may arise in adolescence
Etio not related to smoking
Site central > peripheral
Clin hormonal or paraneoplastic symptoms not common
Imaging central well-defined round nodule
endobronchial or peribronchial
Peripheral sharply circumscribed nodule
intraparenchymal
Cytology cellularity high
Cells uniform and round but occasionally spindled
Nuclei monotonous, round, smooth contours
Salt and pepper (pap)
Nucleoli small and inconspicuous
Cytoplasm moderate, finely granular
eccentric but can be central (giemsa)
eosinophilic (HE), grey-blue (pap), magenta (giemsa)
arch Stripped, branching, fibrovascular strands
may have attached cells
pseudorosettes common
Mol no clinical role for testing (no actionable targets)
Note Typical < 2 mits/2mm without necrosis
Atypical 2-10 mits or with necrosis (usually focal)
mitotic counts not validated procedure for cyto
rarely seen in sputum where cells are dyshesive
Media WSI
Small cell lung carcinoma
Aka SCLC
Etio related to smoking
May arise w TKI resistance in NSCLC
Clin advanced presentation w mets
Malignant effusions, paraneoplastic syndromes
Mets mc brain, liver bone, adrenal
Cytology cells 2-3x size of lymphocyte
Cytoplasm usually scant
Nuclei angulated, moudling (giemsa)
Granular chromatin (pap)
Chromatin may be smeared
May have significant crush artifact
Nucleoli occasional but small
arch crowded, irregular tissue fragments
Discohesive single cells as well as small groups
Background necrotic
IHC (+) NE markers, TTF1, anl p53, high Ki67
Cam5.2 rim and dot-like pattern
IHC (-) HMWCK, p40, p63, CD45, Napsin A
Mol RB1 inactivation and TP53 mtn ubiquitous
DDx Basaloid SCC
Carcinoid[84]
LCNEC[85]
Lymphoma[86]
Metastasis
Media WSI
Large cell neuroendocrine carcinoma
Site peripheral, rarely inolving main airway
Most inoperable at diagnosis
Image irregular tumor borders
expansive growth in peripheral lung
common to have mediastinal lymphadenopathy
Cytology cells size > 3 lymphocytes
Cytoplasm moderate to abundant
Nuclei subtle moulding, if present
Chromatin can be granular or coarse
Nucleoli large or inconspicuous
May show perinucleolar clearing
Background prominent necrosis
Lymphoproliferative diseases
Lymphomas
Pulmonary Langerhans cell histiocytosis
Cytology Langerhans cells cleaved/convoluted nuclei
fine chromatin
long cytoplasmic processes
Charcot leydin crystals
Background eosinophil
IHC(+) CD1a, S100
Erdheim-Chester disease
Mesothelioma
Media WSI epithelioid
Other malignancies
Thymoma
Media WSI type A
Salivary gland-type carcinomas
Media WSI Adenoid cystic carcinoma
Adenosquamous carcinoma
Pleomorphic carcinoma
Pulmonary blastoma
Carcinosarcoma
NUT carcinoma
Thoracic SMARCA4-deficient undifferentiated tumour
Spindle cell tumors
Solitary fibrous tumor
Paraganglioma
Diffuse pleural mesothelioma
Primary germ cell tumours of the mediastinum
Primary angiosarcoma of the lung
Pulmonary and thoracic metastases
Media WSI Metastatic adenoid cystic carcinoma
WSI Metastatic adenoid cystic carcinoma
WSI Metastatic adenoid cystic carcinoma
WSI Metastatic adenoid cystic carcinoma
WSI Metastatic anaplastic meningioma
WSI Metastatic chordoma
WSI Metastatic colorectal adenocarcinoma
WSI Metastatic endometrial clear cell carcinoma
WSI Metastatic meningioma
WSI Metastatic angiosarcoma
WSI Metastatic small cell carcinoma
WSI Metastatic renal cell carcinoma ─ clear cell type
WSI Metastatic urachal adenocarcinoma ─ enteric type
WSI Metastatic prostatic adenocarcinoma
WSI Metastatic triple-negative breast carcinoma
WSI Metastatic pleomorphic adenoma
WSI Metastatic urothelial carcinoma
WSI Metastatic Melanoma
Infections
Herpes simplex virus
Mycobacterium
Media WSI
Blastomyces
Cytology thick-walled yeast forms
Broad based budding
Media pathoutlines
Coccidiodomycosis
Cytology round endospores contained wi large spherules
Spheules 100μm, endospores 20μm
Spherules have a crushed appearance
Paracoccidiodomycosis
aka South American blastomycosis
site lungs & mucocutaneous sites
epid mc mycosis in Latin America
can affect healthy pt
clin resembles TB
cytology GMC ship's wheel[87]
Sporotrichosis
Site lung uncommon
Cytology yeasts resemble Cryptococcus, Histoplasma, Candida
culture/molecular needed for dx
Aspergillus
Trans spore inhalation
Clin normal host no sequelae
Cavitary lung dz aspergilloma
Asthma/CF ABPA[88]
Immunocompromised invasive aspergillosis
cytology narrow (2-4μm) septate hyphae
Media WSI With Charcot Leiden crystals
WSI with adenocarcinoma
Mucor
Cytology broad (7-20μm) ribbon-like aseptate hyphae
Haphazard wide angle branching
Media pathoutlines
Cryptococcus neoformans
cytology variably sized yeasts with narrow-based budding
Mucicarmine highlights thick mucoid capsule
Histoplasma capsulatum
cytology clusters of small (2-4μm) oval yeasts within MΦ
Narrow based budding
Pneumocystis Jirovecci
Clin immunocompromised, esp HIV/AIDS
Micro alveolar casts of foamy exudate
GMS Cup-shaped cysts
prominent central dot
does not have budding
Cysts ~RBC size
Strongyloides
Epid immunocompetent < immunodeficiant
Site GI or skin then hematogenously to lung
Cytology notched tail, short buccal cavity
Non-Neoplastic, Non-Infectious Diseases
Sarcoidosis
Granulomatosis with Polyangiitis
Pulmonary Amyloidosis
Pulmonary Alveolar Proteinosis
Etio impaired surfactant clearance
Immunodeficiency, autoimmune, exposures
Radio crazy paving pattern
Cytology large, acellular, eosinophilic, proteinaceous blobs
Pulmonary MΦ filled w PAS+ material
Organizing Pneumonia
Cytology masson bodies, pulmonary MΦ hemosiderin
Spindled fibroblasts embedded in collagen
Reactive pneumocytes
Neoplastic
Adenocarcinoma
─ Cyto ─ Breast
Benign
Ductal hyperplasia
Cytology Hypercellular, 3D fragments
Variable cellular dyshesion
2nd cell population (ME cells)
Cells display polarity & streaming
Fibroadenoma
Cytology staghorn epithelial clusters
Naked bipolar cells in background
Metachromatic stroma
Background bipolar naked nuclei of ME cells
Lactating adenoma/lactational change
Etio hormonal stimulation during pregnancy or lactation
Cytology Hypercellular
Fragile lipid-rich cytoplasm so nuclei are often stripped
Prominent nucleoli
ductal cells w prominent nucleolus
vacuoles wi cytoplasm and background
Gynecomastia
Def enlargement of male breast
secondary to stromal and ductal proliferation
clin majority of male breast lesions undergoing FNA
Apocrine cyst
Fat necrosis
Media WSI
Apocrine metaplasia
Cytology hypercellular, dyshesive cells
No ME population
Note need extreme atypia for carcinoma w apocrine diff
Subareolar abscess
Aka Zuska s disease
Etio smoking-related SMOLD
Cytology wall to wall PMNs
Keratinaceous debris
scattered squamous cells, some anucleate
histiocytes, multinucleated foreign body giant cells
Intramammary lymph node
Cytology hypercellular, dyshesive cells
lymphoglandular bodies
tingible-body macrophages
Malignant
Medullary Carcinoma
Media WSI
Ductal carcinoma
Media WSI WSI WSI WSI WSI WSI WSI
Lobular carcinoma
Micro Hypocellularity secondary to associated fibrosis
Small tumor cell size
Nucleus membrane irregularity, coarse chromatin
Intracytoplasmic lumen (mucin)
Note Accounts for most false-negative breast FNAs
Colloid carcinoma
Cytology hypercellular
large amounts of mucin in background
cytologically-bland cells in mucin
lacking 2nd cell (ME) population
mucin best seen on air-dried, Diff-Quik stained smears
Tubular carcinoma
Cytology Generally cellular
tightly-cohesive tissue fragments
minimal nuclear atypia
fragments display bent configurations ("teardrop")
no ME population
Adenocarcinoma
atypia not required
dyscohesion
lack of myoepithelial cells
hypercellular
False positives
tubular adenoma
lactating adenoma and lactational change
papilloma
Fale negatives
sclerotic leions
lobular carcinoma
well-differentiated carcinoma (tubular carcinoma)
Ductal hyperplasia
Hypercellular specimen
Densely-cellular, 3-dimensional fragments
Variable cellular dyshesion
Fragments should contain 2nd cell population (ME cells), visible in alcohol-fixed material
Cells within fragments display polarity and streaming
Fibroadenoma
Classic FNA findings
Complex branching fragments of ductal epithelium ("antler horns")
Naked bipolar cells in smear background
Metachromatic stroma
Pitfalls
Hypercellularity and architectural complexity within fragments in cases with ductal hyperplasia
Cellular dyshesion in cases with ductal proliferation
Follow-up
Most cases will undergo elective excision
Correlation with histology valuable in hypercellular cases
Lactating adenoma/lactational change
Hypercellular specimen
May contain numerous loosely-cohesive tissue fragments and intact single cells
Ductal cells with single prominent nucleolus
Numerous vacuoles (fat) within cytoplasm and in smear background (air-dried Diff-Quik)
Diagnostic threshold for malignancy in FNA of pregnant/lactating patient?
Lobular carcinoma
10-20% of breast carcinomas
Accounts for 75% of false-negative breast FNAs
Hypocellularity (secondary to associated fibrosis)
Small tumor cell size
High-power examination of single tumor cells often reveals
Nuclear membrane irregularity
Coarse chromatin pattern
Intracytoplasmic lumen (mucin)
Colloid carcinoma
Generally hypercellular aspirate
Large amounts of mucin in smear background
Small fragments of cytologically-bland cells in mucin lacking 2nd cell (ME) population
Mucin best seen on air-dried, Diff-Quik stained smears
Tubular carcinoma
Generally cellular aspirates
Tightly-cohesive tissue fragments with minimal nuclear atypia
Fragments display sharp, angulated, bent configurations ("teardrop")
Fragments uniformly lack 2nd cell (ME) population
Gynecomastia
Defined as "enlargement of male breast secondary to stromal and ductal proliferation"
Clinical presentation
Bilateral (25%, hormone-related)
Unilateral (75%, drug-related or idiopathic)
25% of cases regress spontaneously
Accounts for vast majority of male breast lesions undergoing FNA and excision
I. Extensive apocrine metaplasia
May be extremely proliferative & cellular in FNA of benign lesions (FCC)
May display dyshesion/single cells
Fragments will not display 2nd cell population
Demand extreme cellularity and nuclear atypia prior to diagnosis of carcinoma in presence of apocrine differentiation
II. Intramammary lymph node
Will yield hypercellular, dyshesive population of cells
False positive diagnosis of lobular carcinoma possible
Diff-Quik stain valuable
Search for lymphoglandular bodies and tingible-body macrophages
Media pathoutlines
─ Cyto ─ Salivary
Normal Salivary Glands
Non-Diagnostic
Criteria insufficient lesional cellls (ideally > 60)
Artifacts (air drying, obscuring blood, poor staining)
Normal gland elements only in the setting of a mass
Non-mucinous cyst fluid wo an epithelia component
Necrotic debris, deveoid of epithellial or inflm cells
Note presence of atypia excludes this category
Mucinous cyst fluid wo epithelial component is AUS
suggestive matrix wo cells is not non-diagnostic
Media pathoutlines
Milan System Atlas
Non-Neoplastic
Media pathoutlines
WSI WSI WSI Abundant amylase crystalloids
Sialolithiasis
Etio Ca phosphate and Ca carbonate stones
Epid extremely rare in kids
Site mc submandubular gland (Wharton s duct)
Parotid gland (Stensen s duct)
Cytology cells hypocellular
metaplastic squames
ciliated or mucinous cells
other admixed stones, coarse calcification
inflammed mucoid background
Absent acinar cells (or scant)
DDx MEC
Acute Sialadenitis
Etio suppurative S aures, Step species
Nonsuppurative viral infections
Epid suppurative adults
Nonsuppurative kids
Site parotid mc
Clin painful
Cytology cells abundant neutrophils, histiocytes
Other necroinflammatory debris (suppurative)
Granulation tissue in later stages
DDX infarcted oncocytic neoplasm
Tumor diathesis in high grade cancer
Chronic Sialadenitis
Etio duct obstruction
Bulimia, trauma, autoimmune, radiation
IgG4-related disease
Site submandibular
Cytology cells hypocellular, small groups of ductal cells
other mild chronic inflammation
fibrotic stromal components
amylase crysalloids, non-birefringent
absent acinar cells (or scant)
DDx basaloid neoplasm more cellular, 3D groups
Granulomatous Sialadenitis
etio response to extravasated ductal contents
infectious mycobacterial, actinomycosis
sarcoid
cytology cells scant acinar, ductal cells, groups of histiocytes
Lymphoepithelial Sialadenitis
etio autoimmune
clin positive anti-SSA, anti-SSB, or RF & ANA titer
Sj gren s manifestations
site parotid glands, submandibular glands
rarely minor salivary glands
cytology cells cohesive sheets of ductal cells
metaplastic squames
nuclei enlarged, reparative changes
lack marked pleomorphism
other germinal center components
absent acinar cells (or scant)
Eosinophilic Sialadenitis
Media WSI
Sialodenosis
Etio non-inflammatory, non-neoplastic enlargement
Clin gradul enlargement, not painful
Cytology cells cellular aspirate
Clusters of hypertrophic acinar cells
Normal acinar architecture
Other background of stripped acinar nuclei
Fibroadipose tissue
Absent cystic or inflammatory features
Neoplastic Benign
Media pathoutlines
Prog 3% ROM
Warthin tumor
Epid 2nd most common SGN, 50-70yo
Etio smoking
Site parotid
Clin doughy painless mass
Cytology Cells uniform oncocytes, small lymphocytes
Cytoplasm oncocytes homogeneous, granular
Well-defined borders
Nucleus oncocytes central, prominent nucleolus
Other dirty proteinaceous background
DDx LESA lack oncocytes and debris
Oncocytoma lack lymphs and debris
Media WSI WSI WSI WSI WSI WSI WSI
Pleormorphic adenoma
Epid most common SGN
Site parotid
Cytology Cells modestly cellular
Biphasic (myoepithelial > ductal)
Myoepithelial cells have a variety of shapes
Ductal cells recap ducts, small cohesive groups
Matrix distinctively chondrmyxoid & fibrillary
Magenta on Romanowky, grey-green on pap
Surrounds each cells, giving troll hair appearance
Nuclei bland in ductal and myoepithelial cells
WSI WSI WSI myoepithelial-rich
Oncocytoma
Epid 50-80yo
Cytology cells sheets and clusters of large polygonal cells
Cytoplasm abundant, homogenenous, granular
Nuclei enlarged, round, distinct nucleolus
Other background clean
Absent nuclear pleomorphism or mitotic figures
Media WSI
Mesenchymal tumors
Lipoma
Cytology cells sheets & clusters
Nuclei small, hyperchromatic, displaced by fat vacuoles
Cytoplasm single large clear vacuole
Other background droplets of lipid
Schwannoma
Cytology cells scant to moderately cellular
Spindle shaped
Nuclei small, dark, bland
Enlarged with ancient change
Nucleoli small or absent
Cytoplasm wispy bipolar cytoplasmic processes
Pale, ill-defined, fibrillary appearance
Other background myxoid appearance (occasionally)
Lymphangioma
Cytology cells hypocellular
Scattered mature lymphocytes
Other watery background with RBCs
Background non-neoplastic acinar tissue
Basal cell adenoma
Media WSI
Neoplastic SUMP Patterns
Media pathoutlines
Cellular Basaloid Neoplasm
Cellular Oncocytic/Oncocytoid Neoplasm
Clear cell features
Suspicious for Malignancy
Prog 35% ROM
Media pathoutlines
Malignant
Media pathoutlines
Acinic cell carcinoma
Epid 2nd mc malignant SGN
Common in kids
Cytology Cells uniform polygonal epithelial cells
Dispersed or loosely cohesive
May adhere to capillaries or make papillae
Nuclei uniform, round, eccentric, distinct nucleolus
Cytoplasm zymogen granules (variable, PASD+)
Background background clean or frothy
stripped nuclei, sometimes lymphs
Other Rarely psammoma bodies
Absent mitotic acitivity, necrosis
ICC NR4A3+
Media WSI
Secretory carcinoma
Epid M = F
Cytology cells cuboidal, polygonal
No lobular arrangement of normal acini
Nuclei uniform, round, centrall located, smooth contours
Fine chromatin, distinct central nucleolus
Cytoplasm indistinct cell membranes, low N:C
Abundant, vacuolated, pale
background proteinaceous material
Absent cytoplasmic zymogen granules
ICC (+) mammaglobin, S100, GATA3
ICC (-) DOG1, myoepithelial markers
Prog indolent
Note very much resembles ACC except no granules
Epithelial-myoepithelial carcinoma
Epid 50-70yo, F > M
Clin localized, slow growing, painless
Cytology cells 2 - 3 : 1 ductal : myoepithelial cells
pseudopapillary groups, sheets, 3D groups
nuclei myoepithelial bland, open chromatin
cytoplasm myoepithelial abundant, clear, glycogen rich
background stripped nuclei (fragile cytoplasm)
other laminated, acellular stromal cores
mol HRAS mutations
Salivary duct carcinoma
Etio most are a transformation of carcinoma ex PA
Epid pak incidence in 60s, M >> F
Clin frequent facial nerve incolvement
Large, infiltrative growth, presents late stage
Cytology cells medium-large, polygonal, overtly malignant
sheets, 3D clusters
Occasional cribriform patterns
Nuclei enlarged, oval, pleomorphic with anisonucleosis
Hyperchromasia and prominent nucleoli
Cytoplasm abundnat & granular ─ oncocytic/apocrine-like
Well-defined cell borders
Other dirty & necrotic background
stripped enlarged nuclei
ICC (+) AR, GATA3, GCDFP-15, frequently Her2/neu too
ICC (-) ER & PR (usually)
DDx MEC squamoid features
Metastatic SCC keratinization
Oncocytic ca lack necrosis
lack ductal features
Note highly prolifertive (Ki-67)
Lymphoepithelial carcinoma
Epid rare, Eskimos and East Asia
60s in USA
Etio EBV in endemic areas, USA non EBV
Clin cervical LAD
Cytology cells syncytial clumps or dispersed
Polygonal to spindle-shaped
Nuclei pleomorphic, vesicular, distinct nucleoli
Cytoplasm moderate to scant
background abundant lymphocytes and plasma cells
Note same cyto as nonk nasopharyngeal ca
Mucoepidermoid carcinoma
Epid most common malignant SGN in kids & adults
Peak incidence 10-20yo
Site most often parotid
Cytology cells mucus cells, intermediate, and epidermoid cells
Absent keratinization
LG more mucus cells, more cystic, mild atypia
HG more epidermoid cells, markedly atypical
ICC (+) p63/p40
ICC (-) AR, GATA3
Mol CRTC1::MAML2
DDx SCC lack of mucus cells
WSI high-grade
Adenoid Cystic Carcinoma
Epid 30 50 yo, F > M
Clin slow-growing, firm mass
Often pw nerve symptosm (eg facial nerve palsy, pain)
Cytology cells Variably cellular, uniform, basaloid
Syncytial sheets with irregular borders
Microcystic sieve-like spaces
Cells surround matrix with a sharp interface
Nuclei bland, oval to angulated, hyperchromatic
Nucleoli indistinct
Cytoplasm indistinct, high N:C
Other matrix acellular, sharp borders, non-fibrillary
magenta on Romanowsky
translucent to pale green on pap
Absent mitoses, necrosis, pleomorphism (except ig HG)
sharp borders around cell groups
ICC (+) CD117
mol MYB::NFIB
prog slow progression, multiple recurrences, late metastasis
Note matrix may be absent in solid variant
Myoepithelial Carcinoma
Cytology Cells cellular aspirate
clusters, sheets, crowded groups
plasmacytoid, spindled, clear, or epithelioid
nuclei variable atypia, depending on grade
background metachromatic stromal material
Small globules and bands with fibrillar edges
Carcinoma ex Pleomorphic Adenoma
Epid 50-70 yo (decade later than PA), F > M
Site parotid
Clin long-standing firm mass with recent rapid growth
Facial nerve palsy or skin involvement at presentation
Cytology cells cellular aspirate
Other Focal component of PA often seen
High grade carcinoma, usually SDC, may be seen
Mol chromosal intabilities underly transformation of PA
Media Milan pathoutlines
nondiagnostic pathoutlines
nonneoplastic pathoutlines
AUS pathoutlines
neoplasm: benign pathoutlines
neoplasm: SUMP[89] pathoutlines
[1] distinguished from lymphocyte by their nucleoli
[2] irregularly distributed chromatin, parachromatin clearing, nuclear membrane irregularity, loss of polarity, nuclear crowding, anisomucleosis favor malignancy
[3] Serous c
ystadenoma H&E Pap inhibin Glut1
[4] 84M Serous cystadenoma HE PAS Glut1
[5] Serous cystadenoma H&E PAS PASD
[6] Serous cystadenoma Pap
[7] 60F serous cystadenoma Pap
[8] Chylous/yellow/turbid/serosanguineous
[9] MCN HG pap with resection showing invasive adeno
[10] neoplastic mucinous cyst, pap
[11] solid pseudopapillary neoplasm
[12] pancreatic head masses aw duct stricture with downstreeam dual dilation of both ducts
[13] Delicate, foamy or lacey cytoplasm
[14] Adenocarcinoma, includes Pap and HE
[15] segment on pooly diff
[16] segment on well diff
[17] NET G3 with liver met, includes pap diff-quick H&E, synaptophysin, chromogranin PAX8, CDX2, Ki67
[18] Acinar Cell Carcinoma, HE pap BCL10 synaptophysin
[19] intermediate squames w larger nuc, granular chromatin, abundant cytopasm
[20] basal/parabasal cells, nuc larger than intermediate, scant cytopalsm, granuar and dense and high NC
[21] polarized endocervical glandlar cells
[22] benign endocervical glandular cells, s/p hysterectomy
[23] WHO, normal columnar
[24] WHO, normal secretory
[25] WHO, normal ciliated
[26] WHO, glandular cells after hysterectomy
[27] tight cluster of endometrial glandular cells
[28] exodus
[29] endometrial cell, spherical cluster of small cells w dark nuc, scant cytplasm
[30] reactive nuclear enlargement w nucleoli and neutrophils
[31] WHO, inflammation & repair
[32] A & B mature, C immature, D immature w transitional metaplasia
[33] repacement o endocervica cels by squamous cells
[34] Squamous metaplasia, fla sheet of cells w mild variation in nuc size, round-oval nuc, slightly irreg nuc mem
[35] WHO, mature sq metaplasia
[36] immaure sq metaplasai
[37] tubal-llike epithelium
[38] Ie inflm exudate and basophilic granular debris
[39] WHO, atrophy
[40] atrophy w inflm, parabasal cells w uniformly distributed chr, regular nuc contour, background inflm
[41] WHO, IUD changes
[42] WHO, radiation changes
[43] radiation changes, polychromatic cytoplasm, multinucleation
[44] WHO, actinomyces
[45] WHO, Trichomonas
[46] skewered squamous cells around pseudohyphae
[47] tangles of hyphae and yeast forms
[48] WHO, candida
[49] WHO, gardnerella
[50] Reactive perinuclear halo
[51] WHO, parakeratosis
[52] Atypical parakearatosis, orangeophilic cytoplasm, mild nuc atypia
[53] WHO, hyperkeratosis (leukoplakia)
[54] HO, lymphofollicular cervicitis
[55] WHO, ASCUS bottom ~15 images
[56] ASCUS, poorly formed halos & vacuoles, resembles koilocytes
[57] ASCUS, nucleus 2.5-3x nl intermediate, min nuc hyperchr
[58] ASCUS, single cell w enlarged hyperchr nuc, slight perinuc halo
[59] WHO, ASCH, top ~20 images
[60] rare small cells w high NC, nuc enlargement, hyperchr
[61] single cluster o small cells w high NC, hyperchr, irreg nuc mem
[62] WHO
[63] LSIL, perinuclear cavitation
[64] nuc enlargement and binuc
[65] LSIL, binuc w hyperchr and membrane irregularity
[66] LSIL, koilocytosis and nuc atypia, nuc enlargement, irreg nuc mem and hyperchr
[67] HSIL, high NC, nuc hyperchr, contour irregularity
[68] HSIL, high NC, nuc hyperchr, contour irregularity
[69] HIS, high NC, nuc hyperchr, contour irreg, smaller than LSIL
[70] HSIL single cell w high NC, hyperchr, irreg nuc contour
[71] small cells w high NC, nuc enlargement, irreg nuc mem, hyperchr, absent ncleoli
[72] WHO
[73] atypical endocervical glandular cells, crowded w nuc overlap, feathering, prominent nucleoli
[74] mostly CIS & SCC
[75] Compared to non-keratinizing SCC
[76] Compared to non-keratinizing SCC
[77] Ie the nucleus takees up 2/3 of the cytoplasm
[78] cyst lining cells with enlarged nuclei, finely granular chromatin, and a squamoid or spindle-shaped ( tissue-culture cell ) appearance
[79] Aw FVPTC & NIFTP
[80] A glassy, homogeneous cytoplasmic inclusion
[81] Referred to as endoplasmic ectoplasmic demarcation
[82] prominent nucleoli, Predominantly discohesive, Monotonous primitive cells
[83] Can be mistaken for basaloid carcinoma, ICC needed
[84] lower grade, less necrosis & mitosis
[85] more abundant cytoplasm, Prominent nucleoli & cell borders
[86] more dyscohesive, Lymphoglandular bodies more dyscohesive, Lymphoglandular bodies
[87] yeast forms budding off from parent yeasts
[88] allergic bronchopulmonary aspergillosis
[89] salivary gland neoplasm of uncertain malignant potential